The purpose of this handbook is to analyze clinical, personal and behavioural features of children with multidisability in order to guide the therapeutical and educational choices of operators and families, thus guaranteeing a decent life to every patient.
Before turning to a punctual analysis of every single characteristic, we believe it is very important to outline the clinical picture that qualifies multidisability as a specific entity.
"Multidisability is not a mere aggregation and coexistence of limitations in the same person. It is rather a permanent interaction between pathologies, limitations and disabilities in a dynamic system affected by the internal and external environment of the subject him/herself." (Piccioni, 2005).
Bearing this principle in mind, we have compiled some useful and practical suggestions for therapists, operators and parents taking care of multidisabled children all over world – with a particular focus on developing countries.
Coping with disabled children and all the motor, mental and behavioural implications of their clinical picture necessarily entails different types of analyses. Taken together, the results of such analyses contribute to outline every little patient's world as a whole, unique reality.
This dissertation reports some of our most representative cases and provides a list of questions to gain a deeper understanding of the issues described in each chapter. The introduction of such elements is aimed at supporting trainers in their critical task of effectively turning basic rehabilitation theories into positive practices.
Because of its key role in both the care-giving and educational domain, family need constant support and guidance and is at the very heart of our work. Tratto dall'Introduzione dell'Autrice
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
EducationSubtopic
Essays in EducationChapter 1
Multidisability in children
1.1 What is multidisability
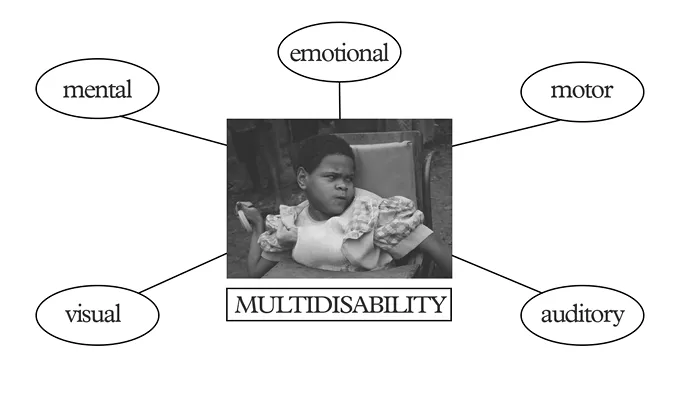
Multidisability refers to a clinical picture grouping various disabilities that depend on the same cause which determines a concurrent reduction or loss of different abilities, with the consequent impairment of the level of autonomy that each disability in itself would imply.
This does not mean that multidisability is to be considered as the sum of two or more disabilities, namely of motor, mental, emotional, visual and/or auditory kind. Rather, it is to be considered as a clinical picture in itself, a manifestation of diffuse encephalic disturbances involving different areas of the Central Nervous System and hence different functions.
In this work we will therefore focus on subjects with in-born severe encephalopathy occurred before, during or after birth.
The disease can have a different impact on families according to whether the cause is known – for instance, severe hypoxemia (i.e. a lack of oxygen in the brain), intracranial haemorrhage whose signs are visible since birth, or still head trauma occurred after birth, even in the first months of life – or not. In the latter case, pathological signs gradually emerge during the first year of life and the clinical picture can either be attributed to genetic damage or remain unknown. Each starting point determine different reactions within the environment in which children live that will influence their future life.
Identifying typical features of multidisability implies avoiding a generic definition of this specific clinical picture that is generally severe, especially at motor level.
Such features vary widely according to two key factors: the extent to which the lesion affects motor, mental, sensory and relational functions; and, above all, the potential acquisition of autonomous motion and self-care and of an adequate level of communication, which is peculiar to single individuals.
As far as autonomy and communication are concerned, we will therefore provide a specific outline of the various clinical pictures taking into account the complexity of the situation and the possible negative interferences due to a reduction in the children’s skills. We will also mention the emergence of other possible medical complications such as epilepsy, breathing diseases, gastro-oesophageal disturbances, obesity, and behaviour disorders such as autism secondary to cerebropathy, inappropriate behaviour responses, introversion and sleep disorders (Fig. 1).

Fig. 1 – A child with multidisability isolating from her context
These problems depend on the type and level of family and social acceptance multidisabled children experience and on the lack of esteem they perceive, especially when their disabilities are not severe and they show a high level of awareness. Such situation can lead to conduct disorders.
1.2 Motor and mental multidisability


Fig. 2 Fig. 3
Motor and mental multidisability is the most frequent picture and is generally due to early birth or perinatal hypoxemia (Fig. 2). Microcephaly (see Glossary) is almost always the clear manifestation of its severity (Fig. 3).
The mental disturbance is the most severe impairment. Indeed, motor disability in itself, though severe, may be partially treated, and the limitations to the development of communication and functionality stemming from it may be overcome by modern techniques in industrialized countries (Fig. 4).

Fig. 4 – A touchscreen helps restoring the grip function
The harsh environmental conditions typical of developing countries sharpen survival instinct and motivation, pushing people to invent new – often incredible – solutions. In fact the lack of means spurs the autonomous search for expedients aimed at overcoming the limits of communication and fosters the development of motor skills and the acquisition of greater functionality (Fig. 5-6).
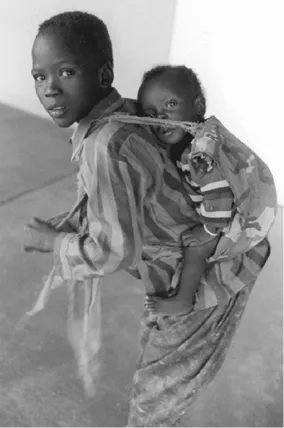
Fig. 5 – A spastic African child carried on the back: this position is the most suitable to prevent hip dysfunctions and is hard to reproduce even with rigid and advanced tools

Fig. 6 – Two rudimentary wooden crutches allow children to walk long distances on rough grounds
However, it is a fact that severe motor disability hampers autonomous motion and self-care.
When intellectual impairment adds to motor disability forecasting, task-planning or autonomous decision-making are severely compromised. In some cases, however, subjects show a significant adaptation degree and get to develop simple but unexpected skills tending towards autonomy.
On the other hand a passive state may arise, making it difficult to understand the child’s real potential.
During the various phases in the life of physical and mental disabled children, growth and the consequent increase in weight may pose other problems (Fig. 7).

Fig. 7 – A girl with physical and mental disorders worsened
by weigh increment
by weigh increment
The first critical phase occurs between 5 and 6 years of age if movement is not activated by appropriately trained staff, namely counsellors, therapists and the family. Muscle and tendon retractions in the knee and plantar flexors, thigh adductors, pronators of forearms (Fig. 8) may be by associated to severe scoliosis and a consequent asymmetry of the trunk, especially when the motor picture is critical (Fig. 9).


Fig. 8 Fig. 9
Then deformity becomes the main problem, its most severe manifestation being hip displacement which is more frequen...
Table of contents
- Acknowledgements
- Index
- Preface
- Introduction
- Chapter 1 Multidisability in children
- Chapter 2 Assessment of multidisability
- Chapter 3 Diagnosis and prognosis
- Chapter 4 Treatment plan
- Conclusion Social life as the final aim for the inclusive process
- Glossary
- Bibliography
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Multidisability by Alda Pellegri in PDF and/or ePUB format, as well as other popular books in Education & Essays in Education. We have over 1.5 million books available in our catalogue for you to explore.