![]()
1
Classifying reactions to stress and trauma
Example 1: You are driving down a busy highway on a rainy day and your tire has a blowout. Your first response is one of action, pulling the car over to the side of the road while avoiding a collision with other cars. Once safely stopped, you realize that your heart is pounding, you feel like you have been kicked in the stomach and you are sweating and trembling.
Example 2: You are barely making ends meet with a part-time job and college bills to pay. You have too much to do and are worrying about an upcoming exam that is very important for your future career. You haven't been sleeping well for the past month and are constantly worrying about completing all your work. You rush into your job about 10 minutes late and the boss says, "That's one time too many. I just can't have you coming into work late. I'm going to have to let you go." You feel the blood leave your face and panic rise in your chest.
Example 3: You and your partner have been planning your wedding. Although you want an event that is special, all of the planning is beginning to feel a bit out of control with all of your other responsibilities. The caterer just went out of business and some of the bridesmaids' dresses came back in the wrong sizes. All of the invitations still need to be addressed but your boss just asked you to take on a project at work that will have you working in the evenings for the next two weeks. You have been experiencing headaches every afternoon and now you feel like you are coming down with a cold.
Example 4: You moved to a new town, don't know anyone, and have gotten lost several times trying to find your way around. You are feeling lonely and disconnected from your old friends. Although you think the move might turn out well eventually, all of the usual routines have changed and even getting a haircut or a dentist appointment is stressful because you don't know where to go or whom to choose. You feel irritable and your stomach has been bothering you.
Example 5: You are peacefully asleep in your bed when suddenly you are awakened by a voice that says, "I have a knife, so don't make any noise." You wonder if you are having a nightmare but as you awaken more fully, you feel the point of the knife at your throat. You begin to hyperventilate as you experience complete terror. You feel frozen both mentally and physically.
All of these are examples of stress, negative reactions to environmental stressors. Stressors may be positive (a promotion at work, a new baby) as well as negative. The stress response is a combination of physical reactions, thoughts (cognitions), emotions, and behaviors. In recent years, the study of stress has focused on the effects of stress on health, and a whole branch of psychology has emerged as health psychology. In the previous examples, only the first and fifth examples might represent traumatic stress. In the first example, the flat tire, some people might not consider the event traumatic because disaster was averted. Someone else might consider the event traumatic because of memories of a prior experience with a car accident, or an appraisal of imminent danger, and accompanying fear. In other words, stress and trauma may depend on how a person appraises the situation and on her or his own emotional reactions. The fifth example is an event that nearly everyone would find traumatic—a sudden, unexpected, life-threatening assault.
The primary focus of this book will be on traumatic stress, those events beyond daily hassles, beyond normal developmental life challenges, beyond more stressful and challenging circumstances such as divorce, losing a job, serious illness, or financial problems. This book will focus on events that are life threatening (and/or threatening to "self" as is the case with incest or other intimate assaults) and that are accompanied by intense fear, helplessness, or horror. Traumatic stressors frequently result in psychological symptoms of a more significant nature than more common stressors and may result in psychological disorders for many people who experience traumatic stress. This chapter will focus on the various psychological disorders that may result from traumatic stress. The next chapter will examine the prevalence of these most serious types of stressors. The remaining chapters will focus on theories of traumatic stress response, variables that affect symptoms and recovery, and treatment.
Reactions to stressful and traumatic events: Symptoms and diagnoses
Immediate reactions
Life stressors can be minor (irritating daily hassles such as waiting in line or commuting in traffic) or major (divorce, death of a loved one); they can be acute (physical injury, moving to a new home) or chronic (living in a dangerous environment, poverty). In response to stressors, people typically have emotions, thoughts (cognitions), physical reactions, and behaviors that correspond to the severity and chronicity of the stressors. For example, while anticipating or giving a speech in front of an audience, many people will experience physical symptoms such as dry mouth, "butterflies" in the stomach, or racing heartbeat. They may have trouble focusing their thoughts or have ruminative or catastrophizing thoughts ("I'm going to sound stupid"). Behaviorally, people who are anxious about performance may stammer or engage in nervous mannerisms. Emotions may include anxiety, irritability, or fear. However, shortly after the speech is finished, most people return to normal very quickly. The stress is over.
In response to chronic or cumulative stressors, people also exhibit a range of physical, behavioral, cognitive, and emotional responses that lessen when the stressful situation(s) have stopped. However, the reactions may be much more pronounced and may have lingering effects. As an example, people living in a chronically stressful situation may develop more generalized thoughts about their own helplessness, or may ruminate about the causes of the situation in a nonproductive manner. They may develop more serious emotional responses that could be diagnosable as depression, anxiety disorders, or chronic anger. They may attempt to cope behaviorally with the situation by abusing substances or withdrawing from others. Chronic stress reactions may contribute to illness and physical disorders. When the stressful situation abates, the reactions lessen, but poor coping styles and rigid or faulty thinking patterns may have evolved that will be used and abused in future stressful situations. On the other hand, if someone develops new, healthy coping strategies, they may be left stronger and more resilient to face future stressors.
Although the onset and duration of traumatic effects is typically brief, traumatic stress may result in much more dramatic reactions and continuing symptoms. Traumatic or catastrophic events are by their nature, sudden, unexpected, and threatening. At the moment the victim perceives danger, his or her body and mind immediately shift into "survival mode". Our bodies are hard-wired for emergencies through a million years of evolution to respond effectively in the face of imminent danger. When a threat is first perceived, the person responds with an alarm reaction that triggers a number of biological, cognitive, and emotional responses. The autonomic nervous system activates a cascade of biological reactions that produce increases in heart rate, respiration, blood pressure, release of stored sugar, increase in muscle tone, heightened awareness, and narrowing of focus away from unimportant information. The body is preparing for fight or flight. However, it is not always adaptive or even possible to flee or fight. An alternative response is freezing and/or dissociating as a means of survival when escape isn't possible. Freezing may function to avoid the attention of the predator, while dissociation may be the defense of last resort, surrender. Dissociation is an alteration of consciousness in which a person experiences a sense of unreality and detachment from the experience or from her/himself. The biological reaction associated with dissociation and numbing appears to have a different function: the reduction of pain and terror (Perry, Pollard, Blakley, Baker, & Vigilante, 1995).
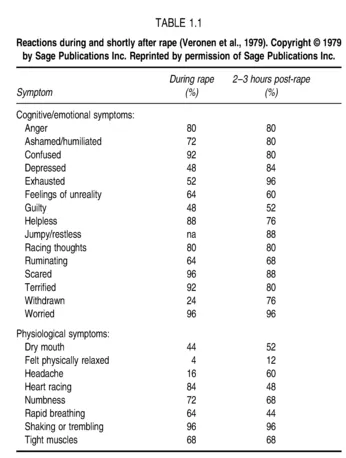
In a study of rape victims (Veronen, Kilpatrick, & Resick, 1979), participants in the research described how they were feeling during the assault. Almost all of the participants reported experiencing multiple emotional reactions during the event (Table 1.1). These victims described a range of reactions including confusion, feelings of unreality, and numbing. In the first few hours after the assault, some reactions increased, particularly cognitive reactions like humiliation and guilt, while others decreased.
Recovery and chronicity
Once the danger has past, the traumatized person now begins the process of recovery. Those who are in pain from injuries or who have dissociated during the event may continue to be shut down emotionally. Some people continue to be emotionally numb for extended periods of time, but most people are flooded with images and
emotions in the aftermath of the event. As they attempt to cope with these strong memories, the victims may begin making efforts to shut off the images and feelings. Too much avoidance, either effortful or dissociative, may lead to prolonged reactions that can evolve into psychological disorders.
The normal course of recovery has been examined with prospective studies, studies of trauma victims beginning at the time of the event and moving forward in time. In the late 1970s, the earliest studies of rape victims were conducted as prospective studies to determine whether and what the psychological reactions were to being sexually assaulted (Atkeson, Calhoun, Resick, & Ellis, 1982; Calhoun, Atkeson, & Resick, 1982; Kilpatrick, Veronen, & Resick, 1979a, 1979b). Rape victims' fear, anxiety, depressive symptoms, sexual functioning, self
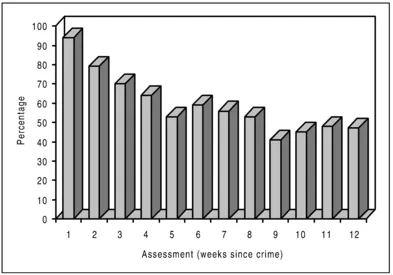
Figure 1.1. Percentage of rape victims with PTSD (from Rothbaum et al., 1992, Journal of Traumatic Stress, Vol. 5, with permission from Plenum Publishing Corporation).
esteem, and social adjustment were examined regularly over at least a 1-year period in groups of rape victims and women who had not been raped. The rape victims reported significantly greater problems in all of these domains compared to the nonvictims although it appeared that the depressive symptoms abated more quickly than the fear and anxiety symptoms. The researchers found that the bulk of recovery occurred within the first 3 months after the event and then little occurred after that.
In the late 1980s and 1990s there were more longitudinal studies that focused specifically on post-traumatic stress disorder of crime victims, motor vehicle accidents or disasters. Rothbaum, Foa, Riggs, Murdock, and Walsh (1992) assessed rape victims weekly for 3 months following their assaults. They found that, similar to the earlier studies, there are very strong reactions initially and gradual recovery over the months that follow. In fact, at 1 week post-rape, 94% of the women assessed met all of the symptom requirements for post-traumatic stress disorder (PTSD), which will be described in detail later in the chapter. At 3 months post-crime, 47% were diagnosed with PTSD (Figure 1.1). When they examined the women who would eventually be diagnosed with PTSD, Rothbaum et al. (1992) found that these women had more severe reactions initially, and that after 1 month they stopped improving. Those who would eventually recover continued to improve throughout the entire study period.
Resick (1988) also compared the reactions of female robbery and rape victims and compared female with male robbery victims over an 18-month period. She found similar patterns although the rape victims had more severe reactions than the female robbery victims did. On the other hand, the female robbery victims had more severe reactions initially than the male robbery victims did, but these differences diminished over time.
Riggs, Rothbaum, and Foa (1995) examined the course of reactions of assault victims and found that, while similar to rape victims, the reactions did not appear as severe. Norris and Kaniasty (1994) examined the recovery of violent crime victims and property crime victims with nonvictims at three time periods: 3, 9, and 15 months post-crime. They assessed a range of emotional reactions and found that while the crime victims showed substantial improvement between 3 and 9 months post-crime, there was no improvement after that. As expected, the violent crime victims reported more distress than the property crime victims, who reported more distress than the nonvictims at each assessment point.
There have been a handful of studies that have prospectively examined reactions to serious motor vehicle accidents or natural disasters (e.g., Blanchard et al., 1996; Green, Grace, Lindy, Glesser, & Leonard, 1990; Mayou, Bryant, & Duthie, 1993; McFarlane, 1988). Generally, these studies have found that people continued to recover over the course of a year. Typically, symptoms are most severe at the earliest time point and the rates of PTSD decrease over time. However, several studies have found a small percentage of people have a delayed onset of PTSD (typically 3-5%). In these cases, those with a delayed onset of full diagnosis did not start with no symptoms; they had a partial diagnosis and then worsened over time until they reached criteria for diagnosis. Blanchard et al. (1996) tracked 132 victims of motor vehicle accidents for 18 months and found that, of the 48 who met criteria for PTSD at 1-4 months post-crime (36%), half had improved at least somewhat by 6 months post-accident, and two-thirds by the 1-year follow-up. There was no significant improvement from 1 year to 18 months post-accident.
While prospective studies are able to show recovery in the early post-trauma period, it is important to remember that the people who participate in these studies may not be representative of all trauma survivors, even those who have experienced the same event. It must be noted that to participate in a study on crime trauma, the victim must have reported the crime to some agency for them to come to the attention of the researchers. People who do not report their crimes to the police, or who suffer in silence for some other reason, may have a different pattern of recovery. In fact, the majority of rape victims do not report their crimes to the police. Also, most of the prospective studies have examined participants for relatively short periods of time, a few months to a few years. There is little research to indicate recovery patterns over a longer period of time.
In one large study of PTSD and other disorders, Kessler, Sonnega, Bromet, Hughes, and Nelson (1995) attempted to examine recovery over a much longer period of time with a retrospective study rather than a prospective study. They asked 5877 people how long it took them to recover from the worst event they had experienced (any of 12 types of events including crime, combat, disasters, etc.) at any time in their lives. These data appear to indicate that recovery occurs beyond the initial 3 months. It also appears from the reports of the participants, that counseling and therapy did not improve the rate of recovery (the number of people who eventually recovered) but those who got therapy recovered sooner. However, this study did not attempt to examine different types of counseling and therapy or even if the therapy was trauma-focused, but merely lumped them altogether.
While advantages of the Kessler et al. (1995) study include the large sample size, the representative sampling of men and women, and the range of traumas examined, because it is retrospective research, it is subject to the vagaries of people's memories. People may not remember accurately how long it took them to recover, especially for events that may have occurred years or even decades earlier. Such research may also pull for recall of specific types of symptoms over others. For example nightmares and flashbacks may be easier to recall than numbing and avoidance. It also must be remembered that when researchers are studying particular disorders and diagnoses, they are engaging in dichotomous thinking—someone is either recovered or they have a full-blown disorder. It is quite possible that someone could be partially recovered. They could have fewer symptoms or less frequent or severe symptoms. It is possible that someone who meets the diagnosis of PTSD (see later in this chapter for specific information on diagnostic criteria), at one point in time and who does not at a later time, might not be recovered. If a person becomes emotionally numb or dissociative and avoids all reminders of the incident, he or she may not have enough reexperiencing symptoms to meet the diagnostic criteria. That person might have partial PTSD, which could be triggered or reactivated at a later point in time.
In spite of these caveats, the prospective longitudinal studies and the larger prevalence studies indicate that some people recover in a reasonable amount of time, usually a few months. Other people stall out, probably early in the recovery process, and develop chronic disorders. The factors that may influence whether and how well someone recovers from trauma will be explored throughout the book. Chapter 2 will examine the prevalence of trauma and the prevalence of chronic disorder in the aftermath of particular stressors. However, first these disorders and other problematic symptoms will be described.
Description of clinical disorders
Although a range of symptoms are considered to be quite normal after a serious traumatic event, when recovery does not occur in a reasonable length of time or if the symptoms grow worse over time, then these symptoms are no longer considered normal. When the psychological symptoms persist following a traumatic stressor and cluster into particular patterns, then it is time to consider whether these reactions have evolved into one or another psychopathological conditions. The remainder of this section will describe various psychological disorders that are frequently observed following trauma. Although almost any disorder might follow in the wake of traumatic experience, there are particular disorders that are more frequent and will be focused on in this chapter. Some disorders, although frequent, will not be described here but can be found in other volumes in this series. They are: mood disorders, substance abuse/dependence, and other anxiety disorders.
Adjustment disorder
Adjustment disorder is a diagnosis that may be appropriate to apply to short-term reactions to a stressor. In this case, the stressor does not need to be unusual or life threatening, but the emotional or behavioral reaction must be in excess of what is typically observed in others who experience the same stressor. The diagnosis of adjustment disorder is not given if the ...