INTRODUCTION
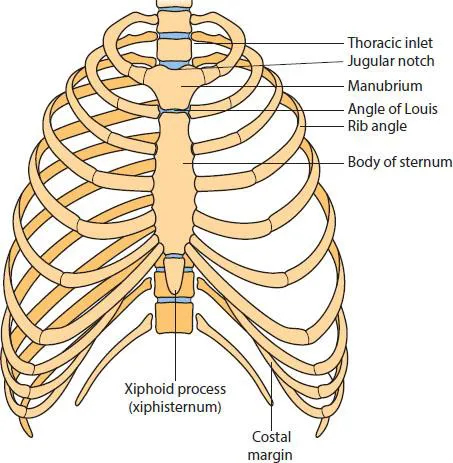
The bony–cartilaginous skeleton of the thorax protects the heart, lungs and great vessels. It is conical, with a narrow inlet superiorly and a wide outlet inferiorly, and is formed of 12 thoracic vertebrae posteriorly, the sternum anteriorly, and 12 pairs of ribs with costal cartilages medially. The thoracic inlet, 10 cm wide and 5 cm anteroposteriorly, slopes downwards and forwards and is bounded by the 1st thoracic vertebra posteriorly, the upper border of the manubrium anteriorly, and the first rib and costal cartilage anteriorly. It transmits the oesophagus, the trachea and the great vessels of the head and neck, and on each side lies the dome of the pleura. The thoracic outlet too is widest from side to side, and is bounded by the 12th thoracic vertebra posteriorly, the 11th and 12th ribs posteriorly, and the costal cartilages of the 7th, 8th, 9th and 10th ribs, which ascend to meet the sternum anteriorly (Fig. 1.1). The diaphragm separates the thorax from the abdomen.
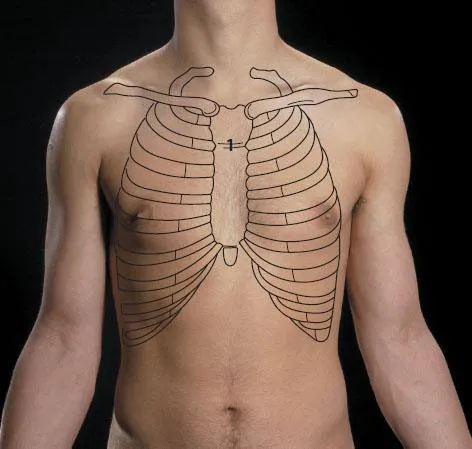
The sternum is a flat bone, palpable throughout its length, with three parts, the manubrium, the body and the xiphoid process (Fig. 1.1). The manubrium is the thickest part, bearing on its upper border the jugular notch between the two lateral facets for articulation with the clavicles. Its inferior border articulates with the body at the palpable sternal angle (the angle of Louis; Fig. 1.2).
This readily palpable protuberance is an important landmark: here the 2nd costal cartilage articulates on the same plane as the 4th thoracic vertebra, the bifurcation of the trachea, and the beginning and end of the aortic arch.
The body of the sternum is some 10 cm long and articulates on its lateral borders with the 2nd to 7th costal cartilages. Behind the body lie the heart valves, in the order from above downwards: pulmonary, aortic, mitral and triscupid (PAMT, Fig. 2.1b, p. 35). The narrow lower end articulates with the xiphoid cartilage, which is cartilaginous in early life and gives attachment to the diaphragm and rectus abdominis.
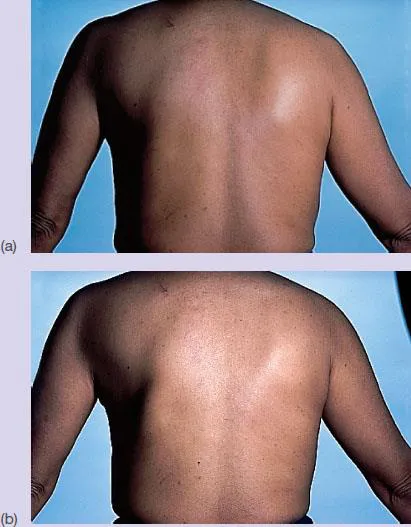
In later life the xiphoid calcifies and can be mistaken for a gastric tumour by the inexperienced clinician. Sternal fractures have become more common because of the frequency of car accidents in which the driver’s chest forcibly hits the steering column – less common with seat belts. Pericardial, cardiac or aortic damage may then follow. A flail chest may also result from multiple rib fractures, when a whole section of the chest wall moves paradoxically during respiration (Fig. 1.3). Air bags and safety belts reduce the incidence of this injury. Although the procedure is less popular nowadays, the sternum is still a useful site for bone marrow aspiration in adults if using the iliac crest is unsuccessful.
The ribs, usually 12 on each side, all articulate posteriorly with the thoracic vertebrae; the upper 7, known as true ribs, articulate through their costal cartilages with the sternum; the 8th to 10th ribs, ‘false ribs’, articulate through their cartilages with the cartilage above; and the 11th and 12th, the ‘floating ribs’, have free anterior ends (Fig. 1.1).
The costochondral and costosternal joints are tiny synovial joints reinforced with fibrous bands. Painful inflammation of these joints, sometimes known as Tietze’s syndrome, can easily be misdiagnosed as cardiac disease. A special form of costochondritis known as the ‘clicking-rib’ syndrome is due to subluxation of a rib casing irritating the underlying intercostal nerve, and the pain it produces is easily confused with abdominal pathology.
A typical rib has a head, neck, tubercle and body (Fig. 1.4). The head articulates with adjacent vertebrae and is attached to the intervertebral disc. The neck gives attachment to the costotransverse ligaments and the tubercle articulates with the transverse process. The flattened curved body has a rounded upper border and a sharper lower border, on the inside of which is the costal groove within which lie the intercostal nerve and vessels.
The 1st, 10th, 11th and 12th ribs are not typical. All articulate with only one vertebra. The 1st rib is short, wide, and has superior and inferior surfaces (Fig. 1.5). The lower smooth surface lies on the pleura; the upper surface has two grooves separated by the scalene tubercle, to which scalenus anterior is attached; the anterior groove is for the subclavian vein and the posterior groove for the subclavian artery and the l...