- 384 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Deep Brain Stimulation and Epilepsy
About this book
Deep brain stimulation has been used effectively for many years to treat patients suffering from Parkinson's disease. Now, neurologists and neurosurgeons are using electric pulse generators to block abnormal activity, i.e. epileptic fits. Promising research results indicate that electric pulses implanted deep in the brain can affect neurocircuitry and help stop oncoming seizures. Supplying a solid background on brain stimulation and its application to epilepsy, Deep Brain Stimulation and Epilepsy provides a historical overview, explores pathogenesis of brain stimulation, discusses animal experiments and human studies, and explores future prospects of brain stimulation for epileptic control. The editor and his team of contributors distill information drawn directly from the literature into one convenient resource.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSection V
Effect of brain stimulation on epileptic seizures: human studies
19
Vagal nerve stimulation: surgical technique
Introduction
Vagal nerve stimulation (VNS) is US Food and Drug Administration (FDA) approved for the treatment of medically intractable partial onset epilepsy in patients over 12 years of age. Efficacy and safety issues have been addressed in several large clinical trials and will not be discussed here.1–4 The device used for VNS is manufactured by Cyberonics (Houston, TX) and includes a pair of helical electrodes (2 mm or 3 mm diameter), a battery-powered generator (Model 101), a tunneling tool, software and programming tools, and supplies for the patient (Figure 19.1). A new generator (Model 102) and lead design was introduced in July 2002. This generator is smaller and incorporates a single pin electrode design to avoid incorrect lead connections.
Background
Indications for vagal nerve stimulation (VNS) include patients with medically intractable partial epilepsy without resective surgical options or those where surgery is contraindi-cated for medical reasons. Contraindications include patients with a history of previous left neck surgery or prior cervical vagotomy. Relative contraindications may include pregnancy, asthma, chronic pulmonary disease, active peptic ulcer disease and insulin-dependent diabetes mellitus. Common adverse effects include coughing, hoarseness, dyspnea and headache. These effects are seen during stimulation and tend to habituate with time. Serious adverse effects have been reported and include vocal cord paralysis, infection, Horner’s syndrome, lower facial muscle paresis and cardiac arrest. Sudden unexplained death has also occurred, but not at a rate different from that of the epileptic population.5 Other mechanical complications can occur, such as lead fracture or generator malfunction.
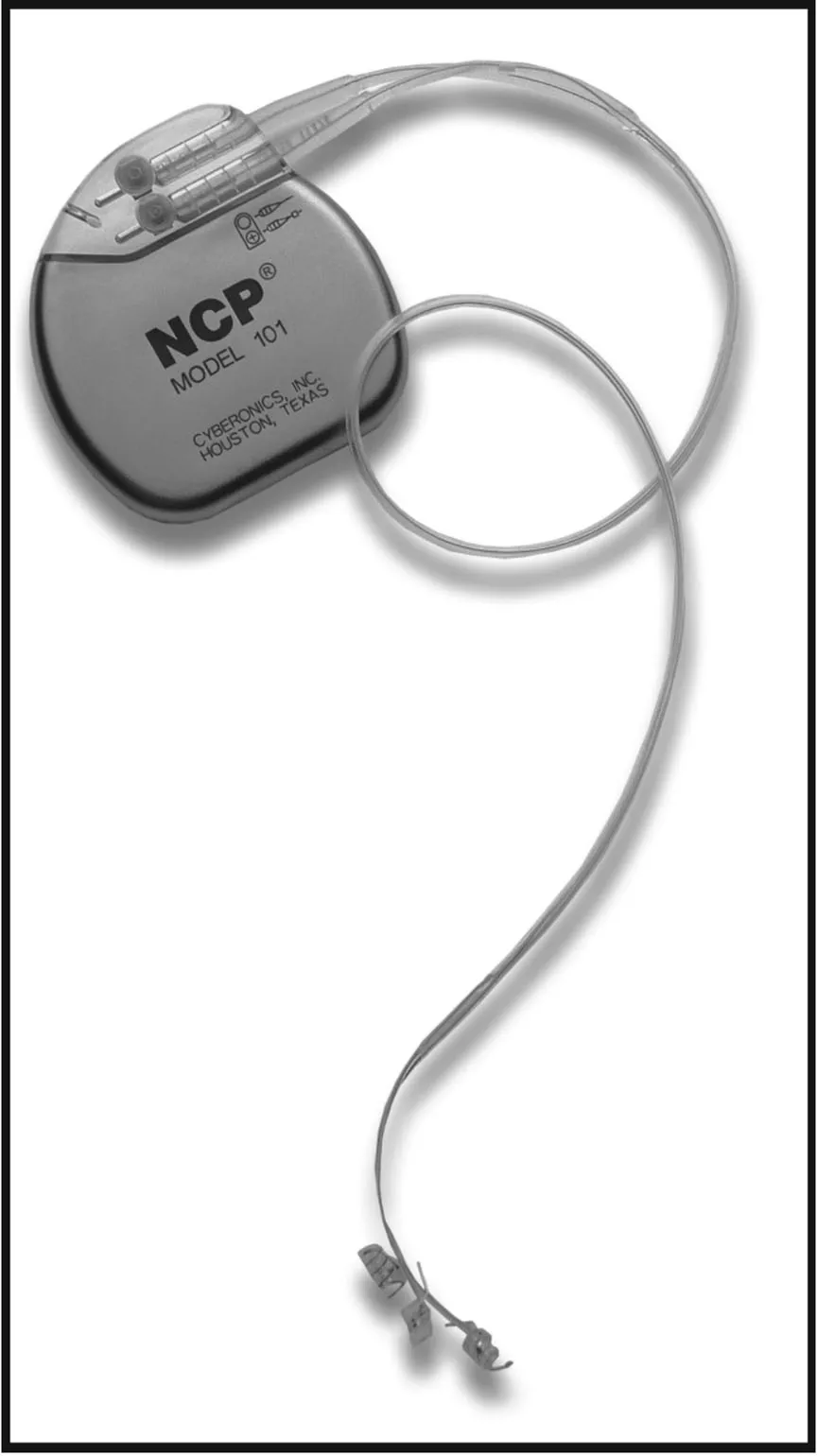
VNS Model 101 generator and electrodes (Cyberonics, Inc, Houston, TX).
Patient selection
Patients with epilepsy uncontrolled by anticonvulsant medications may be candidates for vagal nerve stimulation (VNS). The definition of medically intractable generally includes a description of an adequate drug trial without unacceptable side effects. The exact definition of ‘an adequate drug trial’ is not clear. At our institution, most candidates for VNS have been on many medications without appreciable benefit. Because the efficacy of VNS is not much higher than a new medication trial, it is the author’s opinion that VNS candidates should exhaust medication options prior to consideration for VNS therapy.
Most patients should also undergo a routine pre-surgical evaluation to exclude resective surgical options. This should include inpatient video-EEG monitoring and magnetic resonance imaging (MRI) of the brain with epilepsy protocols (fluid-attenuated inversion recovery sequences and thin-slice coronal T-1 weighted imaging). Other studies might include positron emission tomography (PET) and ictal blood flow studies. The patients are then presented at a multidisciplinary epilepsy conference and the decision to implant a VNS is discussed. The patient is then instructed to keep a seizure diary for three months prior to implantation. Prior to surgery, the patient and family are counseled on post-operative expectations and side effects of stimulation. They are given a videotape of patient information published by Cyberonics.
Although not FDA approved for treatment in the pediatric population, there is growing evidence that VNS is safe and similarly effective in this group.6–8
Anatomy
The vagus nerve is a mixed cranial nerve containing approximately 80% sensory fibers. Efferent fibers innervate the larynx and provide parasympathetic control to the heart, lungs and abdominal viscera. The right vagus nerve innervates the sinoatrial node of the heart while the left innervates the atrioventricular node. In the dog model, stimulation of the right vagus nerve caused more cardiac slowing then the left.9 For this reason, the left human vagus nerve is implanted. Adverse cardiac complications have not been seen, perhaps because stimulation of the nerve can be done on a segment away from the origin of the cardiac branches.
Pre-operative discussion
The patient and family should be educated about the nature of the device being implanted. This includes a discussion of the expectations of the patient and the reality that they will most likely not be seizure-free. They should be counseled that the device will need a battery change in the future. They should be informed that magnetic resonance imaging (MRI) scanning of the body cannot be performed while the VNS electrodes are in place. In addition, the use of diathermy during surgical procedures is forbidden. Routine side effects are discussed (mainly hoarseness during VNS ‘on times’). Complications, such as the risk of infection and the risk of injury to the carotid artery, jugular vein or vagus nerve, should also be mentioned. The patient is also supplied with magnets from Cyberonics which enable the user to turn stimulation on or off . The use of these magnets is uncomplicated and should be explained to the patient and family members.
Surgical technique
The procedure itself is straightforward and could be done by any surgeon familiar with neck anatomy. Neurosurgeons are ideally suited because of the familiarity with epilepsy and their active roles in comprehensive epilepsy centers.
On the day of surgery, the electrode and generator are inspected and tested. A spare generator and electrode should be available in case the primary device fails. Once verified that the equipment is functioning, pre-operative antibiotics are given and the patient undergoes a general anesthetic.
A primary surgeon and assistant participate. The patient is positioned supine on the table with the anesthesia team at the head. The primary surgeon stands at the left side of the neck, his assistant opposite him. The patient’s head is positioned on a ‘donut’ and slightly extended and turned to the right. The surgeon may use a roll under the scapula to help extend the neck. After pre-operative antibiotics are given, the neck and chest is prepped with Betadine scrub and paint solutions. The electrodes are implanted in the left neck by either a ‘carotid’ incision or a transverse ‘collar’ incision. A 3-4 cm incision should be centered at mid-neck level (cricothyroid interval) and on the anterior border of the sternocleidomastoid muscle (Figure 19.2). The skin is incised with a No.10 scalpel and the skin edges undermined with Metzenbaum scissors. The platysma muscle is divided in the direction of its fibers and the deep cervical fascia is opened to identify the sternocleidomastoid muscle. This muscle is mobilized and retracted laterally to expose the neurovascular bundle. This bundle is then incised to expose the carotid artery and jugular vein. The vein is retracted laterally and the main trunk of the vagus nerve is usually found deep between the artery and vein. Approximately 3–4 cm of nerve should be mobilized from surrounding adventitia. Stay sutures in the carotid sheath can be utilized to deliver the nerve towards the surgeon. Mobilization and handling of the nerve should be done with fine forceps. Care must be taken to avoid injuring the main trunk or one of the branches.

Location of incisions: left neck and left axilla.

Subcutaneous pocket: left pectoralis muscle.
Once the nerve dissection has been completed, the left chest incision is marked along the anterior axillary line and opened with a No.10 scalpel. A subcutaneous pocket over the pectoralis fascia is created with sharp and blunt dissection. The pocket must be large enough to accommodate the generator while avoiding strain on the incision line (Figure 19.3).
The electrode array is removed from the sterile package and brought on to the surgical field. Skin edges should be isolated with sterile gauze and the electrode tunneling device passe...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Contributors
- I Historical overview: brain stimulation and epilepsy
- II Pathogenesis of brain stimulation: animal studies
- III Pathogenesis of brain stimulation: human studies
- IV Effect of brain stimulation on epileptic seizures: animal experiments
- V Effect of brain stimulation on epileptic seizures: human studies
- VI Brain stimulation: future prospects
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Deep Brain Stimulation and Epilepsy by Hans O. Lüders in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.