- 168 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Linked by Blood: Hemophilia and AIDS
About this book
Linked by Blood: Hemophilia and AIDS recounts the factors responsible for the widespread infection of people with hemophilia by Human Immunodeficiency Virus (HIV)-contaminated blood and offers a prescription for addressing the challenges of future viral epidemics. The book describes the impact of AIDS on people with hemophilia, their families, and caregivers.
The collection, processing, and distribution of blood in the early years of the HIV epidemic are described, including the failure of regulatory agencies to promulgate effective rules to safeguard the blood supply. The contributions of individuals and organizations that mitigated the epidemic are recognized. Linked by Blood presents recommendations for addressing the myriad medical, social, and economic challenges posed by blood-borne viral infections (AIDS, Ebola, MERS) that periodically sweep through large segments of our population.
- Addresses the challenges of future viral epidemics
- Promotes understanding of the risks and benefits of blood transfusion
- Demystifies HIV/AIDS by explaining how the virus causes disease and is detected and treated
- Covers the factors that led to contamination of the blood supply and contributed to the AIDS epidemic
- Provides background information on hemophilia: who is affected, why they bleed, how it is treated, and what complications can occur
- Discusses the role of regulatory agencies in protecting the blood supply and ensuring the safety of blood and blood products
- Features new proposals to enhance blood product safety and regulate the prices of blood, drugs, and devices that are essential for human health
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
AIDS & HIVChapter 1
The Impact of AIDS on Hemophilia
Abstract
This chapter examines the impact of the acquired immunodeficiency syndrome (AIDS) on individuals with hemophilia and their families. Disease caused by the AIDS virus (human immunodeficiency virus (HIV)) is doubly devastating because it produces a lethal physical illness and contributes to the social isolation of those infected. People with AIDS have recurrent infections requiring frequent physician visits, repeated hospitalizations, and expensive medications; they also experience rampant discrimination and often are barred from attending school and the workplace. The financial liability of hemophiliacs increased exponentially between 1982 and 1992, although government legislative actions provided some relief. Hemophiliacs initiated litigation against blood bankers, pharmaceutical firms, and government health officials in Europe and North America, who were accused of knowingly dispensing contaminated blood and blood products. This chapter details the social, medical, and financial impacts of HIV on the hemophilia community and describes the measures taken to ease their burden.
Keywords
HIV; AIDS; hemophilia; social isolation; Ricky Ray Hemophilia Relief Fund Act; Ryan White HIV/AIDS Program; litigation; contaminated blood
During the 1970s, most individuals with hemophilia began to use clotting factor concentrates because these products dramatically improved their lives and enabled them to enter the mainstream of society. They and their physicians considered these therapeutic materials to be indispensable for the modern treatment of hemophilia. However, the preparation of concentrate required the use of plasma from thousands of donors, and the inclusion of a single plasma donation from one person infected by a virus could contaminate an entire lot of concentrate.
The 1970s also saw the emergence of the gay liberation movement and the appearance of bathhouses and sex clubs that allowed homosexuals to engage in unlimited sexual activity. A single individual infected by human immunodeficiency virus (HIV) could spread this virus to hundreds of partners. Homosexuals were a major source of the plasma used to prepare clotting factor concentrates; during the 1970s, they donated 5–9% of the blood collected by the Irwin Memorial Blood Bank in San Francisco [1]. Concentrate potentially contaminated by HIV was widely used for the treatment of hemophiliacs in the United States and shipped internationally.
Between 1980 and 1992, the Centers for Disease Control (CDC) reported that at least 1928 of the nation’s estimated 15,000 hemophiliacs were infected by HIV, and 1654, or 1 in 10, died of acquired immunodeficiency syndrome (AIDS) [2]. In Canada, 660 of 2427 (27.2%) hemophiliacs became HIV-positive, and 406 died [3]. The worldwide decimation of hemophilia communities was a consequence of the convergence of concentrate therapy for hemophiliacs and HIV contamination of the blood supply that occurred in the United States in the late 1970s.
The impact of AIDS on hemophiliacs and their families was enormous, affecting not only health but also social relationships, education, and work. Prior to the epidemic, people with this disorder lived in the “golden era” of hemophilia [4]. Medical advances had resulted in the availability of commercial clotting factor concentrates that could be infused at home by the person with hemophilia or a family member. These blood products could arrest serious bleeding within minutes, alleviating pain and preventing disability. For the first time, hemophiliacs could maintain satisfactory school attendance, select rewarding careers, and become productive members of society.
AIDS changed everything. People who were unaware they were infected by HIV donated blood, and this HIV-contaminated blood was used to manufacture the clotting factor concentrates used by hemophiliacs. Hundreds of hemophilic men and boys became infected by the virus, and although they had learned to cope with painful muscle and joint hemorrhages before the AIDS epidemic, they now encountered a disease that could affect any organ in their bodies. Almost all developed fatigue, weight loss, and swollen lymph glands. Pneumonia was common, as were fevers and diarrhea. Clinic visits and hospitalizations became frequent, causing major disruptions in work, school, and family life.
The experience of hemophiliacs receiving their care at the Northwestern Center for Bleeding Disorders was fairly typical. In November 1983, 43 hemophiliacs were enrolled there; 33 (77%) had symptoms and laboratory abnormalities consistent with HIV infection [5]. To accommodate these infected individuals, a combined hemophilia and HIV clinic was established to deal with the myriad of new clinical disorders associated with AIDS. A “one-stop” service was provided; each patient was interviewed, examined, and treated by a hematologist and an infectious disease specialist. A nurse-coordinator and social worker rounded out the team; this enabled each patient to receive comprehensive care for hemophilia and HIV infection.
The destruction of the immune system that accompanied HIV infection predisposed to several other disorders, such as decreased blood platelets, cancer of the lymph glands, and progression of chronic viral hepatitis. A low platelet count was observed frequently and was particularly harmful because platelets are needed to prevent bleeding, and their loss can aggravate hemophilic bleeding. Furthermore, the customary treatment for low platelets, a steroid drug, increases the risk of infection, especially in highly susceptible HIV-infected persons. Therefore, the treatment of these patients was problematic. Other therapies, such as intravenous gamma globulin, were effective but were an option for only a few patients because of their high cost [6].
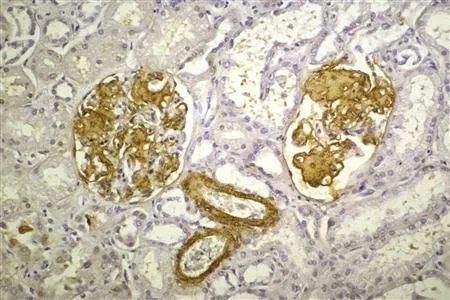
Cancer of the lymph glands occurred in 5.5% of HIV-positive hemophiliacs and was eventually fatal in many patients despite an initial response to chemotherapy [7]. Occasionally, previously rarely seen disorders were encountered. For example, a young man with hemophilia and HIV infection developed an atypical form of tuberculosis. Multiple courses of powerful antibiotics controlled the tuberculosis, but he began experiencing severe fluid retention, with extreme swelling of his face, abdomen, arms, and legs. He became bedridden and eventually died of pneumonia. At autopsy, heavy deposits of an abnormal fibrous protein called amyloid were found in his kidneys. Amyloid levels are increased in the blood of AIDS patients (and amyloid disease has been reported in monkeys with AIDS). Amyloid deposits in the kidneys damage the normal filtering apparatus (the glomeruli and tubules shown in gold in Fig. 1.1), permitting the loss of normal proteins from the blood and causing fluid retention; this was the cause of the patient’s swelling [8].
Almost all of the patients attending the Northwestern Hemophilia Center were exposed to the hepatitis viruses that contaminated the clotting factor concentrates available at the time. Laboratory tests for these individuals revealed low-grade inflammation of the liver. However, coinfection with HIV resulted in rapid progression of the inflammation, often culminating in death from liver failure. Multicenter studies report that HIV infection increases the risk of end-stage liver disease more than eightfold [9,10]. Some of these patients were candidates for liver transplantation, but even in those with a successful transplant, long-term treatment with powerful antirejection medications was required. These drugs were expensive and had a variety of unpleasant side effects.
Other patients developed infections with organisms that were previously considered exotic. An HIV-infected patient had acute onset of severe headaches and visual impairment, followed by muscle paralysis. A brain biopsy showed progressive multifocal leukoencephalopathy (PML), a rare infectious disease of the brain caused by the J-C virus. There was no treatment for this infection, and the patient died within a few weeks. Several years later, his 26-year-old hemophilic nephew developed AIDS and also died of PML.
Hemophilic men were warned that sexual exposure to HIV posed a risk to their wives. Accepting a prohibition on unprotected sex was especially difficult for young couples wanting to start families. In vitro fertilization was not an option; at the time, no method for sterilizing semen was available that would kill the virus but spare the sperm.1 This meant that couples had to delay starting families indefinitely, which was a great disappointment to many.
Even the treatment of HIV was problematic for some patients. Antiviral drugs often caused nausea, fatigue, and headache, as well as anemia and discoloration of the skin and nails. Another distressing side effect was the accumulation of large amounts of fatty tissue around the neck and upper back. This condition, called lipodystrophy, could be very disfiguring. Although most patients were able to continue working despite the ugly burden, some needed surgery because the mass of tissue became so large that they could no longer button their collars.
Social Impact
When AIDS first came to public attention, it was considered to be a medical oddity because the disease outbreak was largely restricted to the male homosexual communities of New York, Los Angeles, and San Francisco [11]. However, as the number of cases rapidly escalated, AIDS patients soon filled hospital wards in these cities at an alarming rate. Public health workers were concerned that the epidemic would spread from homosexuals to other population groups, and that those who became infected would be subject to social discrimination. Homosexuals have often been targets of intolerance; when AIDS, a disorder predominantly affecting homosexuals, was discovered in hemophiliacs, they encountered similar prejudicial attitudes.
Because the risks of contact with HIV-infected persons were unknown at the time, the National Institutes of Health (NIH) issued broad warnings about exposure to saliva, tears, and other bodily fluids. As an unintended consequence of this action, the general population came to fear proximity to persons with hemophilia and sought to avoid direct and indirect contact with them and their family members. Ryan White, a young man with hemophilia and AIDS, reported that people would not sit near him in restaurants and refused to shake his hand, even in church. He was required to seek separate drinking fountains and restrooms and use disposable eating utensils and trays; in fact, some restaurants even threw away his dishes [12]. After White was diagnosed with AIDS, many parents and teachers in his community feared that he might infect other children, and they signed a petition encouraging school leaders to ban him from returning to his classroom. After an 8-month legal battle, he was finally allowed to attend school—only to be shunned by his classmates and harangued with epithets such as, “we know you’re queer.” White’s supporters were called homosexuals and threatened with death. Windows in his home were broken, the tires of the family car were slashed, and he and his family had to relocate to another town [13]. After these events were reported in the press, Ryan White was interviewed frequently and became a spokesperson for hemophilia and AIDS education. He appeared on national television with celebrities such as Elton John and was quoted in newspapers. He died of AIDS in 1990 at age 19.
In Florida, the local school board refused to allow the three Ray brothers, all of whom had hemophilia and HIV, to attend their public school. The family mounted a legal appeal, but 1 week after the school board action was overturned by a federal co...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Preface
- Acknowledgments
- Introduction
- Chapter 1. The Impact of AIDS on Hemophilia
- Chapter 2. What Is Hemophilia?
- Chapter 3. Blood: Vital but Potentially Dangerous
- Chapter 4. The Human Immunodeficiency Virus
- Chapter 5. Hemophilia: An Affinity for Blood
- Chapter 6. Blood as a Vehicle for the Spread of AIDS
- Chapter 7. A Full-Blown Epidemic
- Chapter 8. The Institute of Medicine Study
- Chapter 9. A Summary of Factors That Enabled the Epidemic
- Chapter 10. Contributions That Mitigated the Epidemic
- Chapter 11. Hemophilia: Past and Present
- Chapter 12. A Prescription for the Next Health Care Crisis
- Further Reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Linked by Blood: Hemophilia and AIDS by David Green in PDF and/or ePUB format, as well as other popular books in Medicine & AIDS & HIV. We have over 1.5 million books available in our catalogue for you to explore.