Transcatheter Mitral Valve Therapies
- English
- ePUB (mobile friendly)
- Available on iOS & Android
Transcatheter Mitral Valve Therapies
About this book
TRANSCATHETER MITRAL VALVE THERAPIES
An essential survey of the advancing field of transcatheter mitral valve repair and replacement
Minimally invasive transcatheter therapies have revolutionized the treatment of structural heart disease. Greatly improving outcomes for higher-risk patients, transcatheter aortic valve replacement is now established as a safe and effective alternative to invasive surgery. The mitral valve, however, poses further challenges. Contending with one of the heat's most anatomically and pathologically complex components, practitioners and engineers have yet to perfect a stream-lined, widely deliverable therapy—though they are getting closer and closer to this goal.
Transcatheter Mitral Valve Therapies provides a far-reaching survey of the field of mitral interventions in its current state. Highlighting the stumbling blocks preventing transcatheter mitral valve replacement's widespread adoption, the book's international group of contributors discuss the improvements to be made in repair and replacement procedures, as well as the adjunctive use of imaging and pharmacologic therapies. This ground-breaking text:
- Provides detailed explanations of transcatheter repair, transcatheter replacement, and adjunctive procedures
- Features chapters on the use of imaging to aid in patient selection, procedure planning, and intra-operative guidance
- Discusses the importance of minimally invasive approaches for mitral valve repair
- Examines anticoagulation following transcatheter mitral valve interventions
- Outlines the possible future of transcatheter mitral valve therapy
Transcatheter Mitral Valve Therapies is an important, up-to-date resource for interventional cardiologists, as well as all clinical researchers and practitioners seeking information on this vital and developing treatment.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
1
The Pathology of Mitral Valve Disease
1.1 Introduction
1.2 General Anatomy of the Mitral Valve
1.2.1 Mitral Annulus

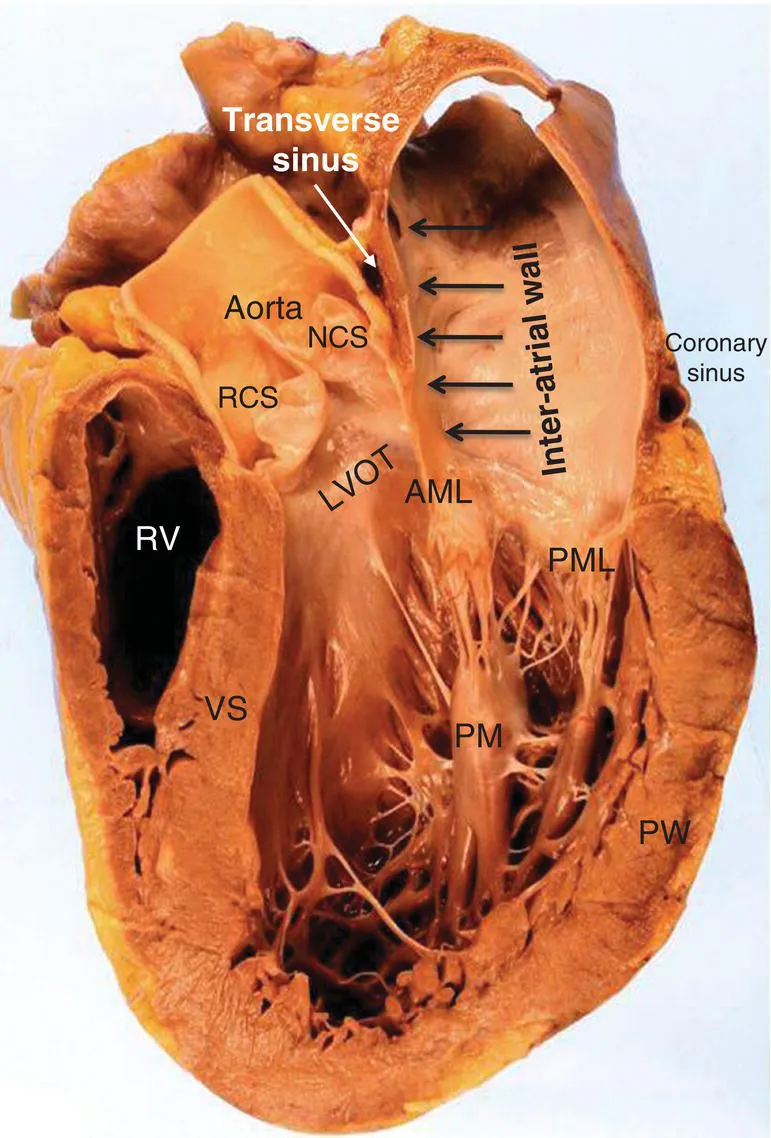
Table of contents
- Cover
- Table of Contents
- Title Page
- Copyright Page
- List of Contributors
- Introduction—The Mitral Book
- 1 The Pathology of Mitral Valve Disease
- 2 The Importance of Minimally Invasive Approaches for Mitral Valve Repair
- 3 When to Intervene—Should Surgical Guidelines Apply to Transcatheter Techniques in Treating Mitral Regurgitation?
- 4 Transcatheter Mitral Valve Therapies
- 5 CMR Assessment of Mitral Regurgitation
- 6 CT Planning for TMVR and Predicting LVOT Obstruction
- 7 General Principles and State‐of‐the‐Art Echocardiographic Evaluation of the Mitral Valve
- 8 Intraprocedural Echocardiography for MitraClip
- 9 Intraprocedural Echocardiography for Transcatheter Mitral Valve Replacement
- 10 Transcatheter Repair
- 11 MitraClip™ for Secondary Mitral Regurgitation
- 12 The Edwards PASCAL Transcatheter Valve Repair System
- 13 The Development of a Novel Percutaneous Treatment for Secondary Mitral Regurgitation—The Carillon® Mitral Contour System®
- 14 A Fully Percutaneous Mitral Ring
- 15 Transcatheter Mitral Cerclage Annuloplasty
- 16 The Transapical Off‐Pump Mitral Valve Repair with the NeoChord Implantation (TOP‐MINI)
- 17 AltaValve™—A Transcatheter Mitral Valve Regurgitation Treatment Technology
- 18 The ARTO Transcatheter Mitral Valve Repair System
- 19 Transcatheter Mitral Annuloplasty
- 20 Transapical and Transseptal Access for Transcatheter Mitral Valve Replacement
- 21 Mitral Valve‐in‐Valve and Valve‐in‐Ring Therapies
- 22 Edwards SAPIEN in Native Mitral Annular Calcification (MAC)
- 23 Transcatheter Mitral Valve Replacement
- 24 TIARA Transcatheter Mitral Replacement System
- 25 Caisson Transcatheter Mitral Valve Replacement System
- 26 Transcatheter Mitral Valve Replacement with the CardiAQ‐Edwards and EVOQUE Prostheses
- 27 Intrepid
- 28 Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction (LAMPOON)
- 29 Use of Alcohol Septal Reduction Therapy to Facilitate Transcatheter Mitral Valve Replacement
- 30 Direct Transatrial Approach with Resection of the Anterior Mitral Leaflet to Prevent Outflow Tract Obstruction
- 31 Transcatheter Closure of Mitral Paravalvular Leak
- 32 Management of Iatrogenic Interatrial Septal Defect—To Close or not to Close?
- 33 Antithrombotic Therapy in Transcatheter Mitral Valve Intervention
- Index
- End User License Agreement
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app