Introducing an essential new practical atlas for dental students and clinicians alike! The Color Atlas of Oral and Maxillofacial Diseases provides comprehensive, practical information on the most common oral and maxillofacial diseases and disorders. This new text uses a quick-access atlas format to help you easily look up clinical signs, diagnosis, and treatments. Nearly 750 high-quality images accompanied by brief narratives demonstrate exactly what clinical signs to look for – making an intervention as timely as possible. Written by four of the top dental authorities in the world, this concise resource is sure to become a clinical favorite.- NEW! Quick-access atlas format makes it easy to look up clinical signs, diagnosis, and treatment of oral and maxillofacial diseases- NEW! Nearly 750 high-quality radiographs and color clinical photos facilitate the identification of lesions and diseases.- NEW! Comprehensive, focused coverage highlight diseases that may affect the oral and maxillofacial regions.- NEW! Full-color design and illustrations.- NEW! Logical organization reflects the sequence in which content is generally presented to predoctoral students.- NEW! Expert Consult TM eBook version included with purchase allows you to search all of the text, figures, and references from the book on a variety of devices
eBook - ePub
Color Atlas of Oral and Maxillofacial Diseases - E-Book
Color Atlas of Oral and Maxillofacial Diseases - E-Book
- 544 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Color Atlas of Oral and Maxillofacial Diseases - E-Book
Color Atlas of Oral and Maxillofacial Diseases - E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaSubtopic
Odontotecnica1
Developmental Defects of the Oral and Maxillofacial Region
Cleft Lip and Palate
Fig. 1.1
Cleft lip (CL) is a common congenital anomaly that is caused by defective fusion of the medial nasal and maxillary processes during embryologic development. Approximately 80% of cases are unilateral and 20% are bilateral. Cleft palate (CP), which results from failure of the lateral palatal shelves to fuse, often occurs in conjunction with CL, although it also may develop as an isolated defect. CL alone and CL with CP are etiologically related conditions that can be grouped together as CL ± CP (CL with or without CP). CP only (CPO) represents a separate entity from CL ± CP. Orofacial clefting is seen with greater frequency in a variety of specific genetic syndromes, although more often it occurs in a sporadic fashion due to a combination of environmental and genetic factors. Factors known to increase the risk for clefts include maternal smoking, alcohol consumption, and phenytoin usage.
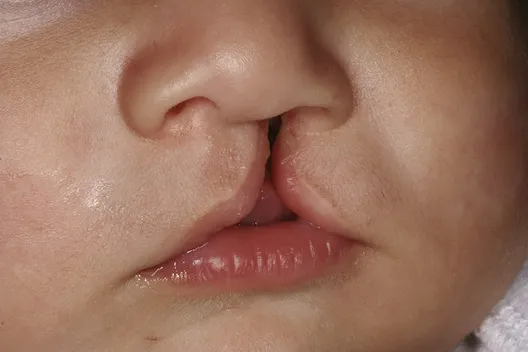
Figure 1.1 Cleft Lip Unilateral cleft of the left upper lip. (Courtesy Dr. Cathy Flaitz.)
The frequency of CL ± CP varies considerably among different racial/ethnic groups. Among whites, the frequency is estimated at 1 per every 700 to 1000 births. The prevalence in blacks is much lower, with a rate of 0.4 cases per 1000 births. In contrast, the rate in Asian populations is about 1.5 times that seen in whites. The highest rate occurs in Native Americans, with a frequency of 3.6 per 1000 births. CL ± CP is more common in males, whereas CPO is more common in females.
Orofacial clefting can result in a variety of problems related to appearance, feeding, speech, hearing, and socialization skills. Management involves a dedicated craniofacial team, which may include specialists in genetics, oral and maxillofacial surgery, orthodontics, otolaryngology, pediatric dentistry, pediatric medicine, plastic surgery, prosthodontics, psychology, and speech pathology. Treatment may require multiple surgeries, with repair of CL usually accomplished around 2 to 3 months after birth and surgical correction of CP undertaken between 6 and 12 months of life.
Bifid Uvula (Cleft Uvula)
Fig. 1.2
During the embryologic formation of the hard and soft palate, the lateral palatal shelves normally fuse in the midline. This fusion begins in the anterior region of the palate and progresses posteriorly to the uvula. If the fusion is not totally completed, then a bifid uvula may occur, which represents the most minimal manifestation of a cleft palate (CP). Sometimes a bifid uvula may be associated with a submucous palatal cleft in which the overlying mucosa is intact but there is a defect in the formation of the musculature of the soft palate. Submucous clefts also may be associated with a notched defect of the midline bone of the posterior hard palate. Bifid uvula is more common than complete CP, with an estimated overall prevalence of 1% to 2%. The frequency is much higher in Asian and Native American populations. In most instances, bifid uvula is an incidental finding that does not cause any problems. If an associated submucous CP is present, velopharyngeal insufficiency may be present, which can result in hypernasal speech. A bifid uvula can be associated with certain genetic conditions, such as van der Woude syndrome and Loeys-Dietz syndrome (hypertelorism, bifid uvula or CP, and aortic aneurysm with tortuosity).

Figure 1.2 Bifid Uvula A midline cleft divides the uvula into two lobes.
Double Lip
Fig. 1.3
Double lip is an uncommon oral anomaly in which there is an excess fold of tissue along the mucosal surface of the lip. It either may be congenital or develop later in life. The upper lip is affected more frequently than the lower lip, although sometimes both lips are involved. The redundant tissue may be seen bilaterally in a symmetric fashion, or it may appear primarily on one side. When the lips are at rest, a double lip may not be noticeable; however, when the patient smiles, the excess tissue will become evident. Double lip occasionally may be a component of Ascher syndrome, which is characterized by the following triad: (1) double lip, (2) blepharochalasis (edema and sagging of the upper eyelid), and (3) nontoxic thyroid enlargement.

Figure 1.3 Double Lip An extra fold of tissue hangs down from the left upper lip.
No treatment may be required for mild forms of double lip. However, more severe examples can be managed by surgical excision of the excess tissue for cosmetic purposes.
Commissural Lip Pits
Fig. 1.4
Commissural lip pits are tiny mucosal invaginations at the corners of the mouth near the vermilion border. Such depressions have been noted in 12% to 20% of the adult population, whereas among children the reported prevalence is only about 0.2% to 0.7%. Although such pits often are considered to be congenital defects, their increased frequency in adult patients suggests that they usually do not appear until later in life. Commissural lip pits occur more often in males than in females.
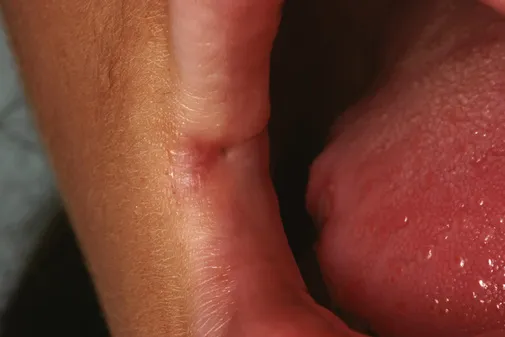
Figure 1.4 Commissural Lip Pit A punctate depression is present at the right lab...
Table of contents
- Cover image
- Title Page
- Table of Contents
- Copyright
- Dedication
- Preface
- Acknowledgments
- 1 Developmental Defects of the Oral and Maxillofacial Region
- 2 Pathology of Teeth
- 3 Pulp and Periapical Disease
- 4 Periodontal Pathology
- 5 Bacterial Infections
- 6 Fungal and Protozoal Infections
- 7 Viral Infections
- 8 Physical and Chemical Injuries
- 9 Allergies and Immunologic Diseases
- 10 Epithelial Pathology
- 11 Salivary Gland Pathology
- 12 Soft Tissue Tumors
- 13 Hematologic Disorders
- 14 Bone Pathology
- 15 Odontogenic Cysts and Tumors
- 16 Dermatologic Diseases
- 17 Oral Manifestations of Systemic Disease
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Color Atlas of Oral and Maxillofacial Diseases - E-Book by Brad W. Neville,Douglas D. Damm,Carl M. Allen,Angela C. Chi in PDF and/or ePUB format, as well as other popular books in Medicina & Odontotecnica. We have over 1.5 million books available in our catalogue for you to explore.