Fetal and Neonatal Secrets by Drs. Richard Polin and Alan Spitzer, uses the success formula of the highly popular Secrets Series to offer fast answers to the most essential clinical questions in fetal and neonatal medicine. With its user-friendly Q&A format, practical tips from neonatologists and fetal medicine experts, and "Key Points" boxes, this portable and easy-to-read medical reference book provides rapid access to the practical knowledge you need to succeed both in practice and on board and recertification exams."Fetal and Neonatal Secrets is a book with an alternative setup that offers answers to a wide spectrum of clinical questions in the field of fetal and neonatal medicine. The book covers both fetal and neonatal medicine, and could be relevant for junior doctors aiming to become obstetricians or pediatricians." Reviewed by: Acta Obstetricia et Gynecologica Scandinavica, January 2015- Get the evidence-based guidance you need to provide optimal care for your fetal and neonatal patients.- Zero in on key fetal and neonatal information with a question and answer format, bulleted lists, mnemonics, and practical tips from the authors.- Enhance your reference power with a two-color page layout, "Key Points" boxes, and lists of useful websites.- Review essential material efficiently with the "Top 100 Secrets in Fetal and Neonatal Medicine" – perfect for last-minute study or self-assessment.- Apply all the latest pediatric advances in clinical fetal neonatology techniques, technology, and pharmacology
- 576 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Fetal & Neonatal Secrets
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Care of the Term Infant
Alan R. Spitzer, MD
1. How is a term infant defined?
The World Health Organization (WHO) defines a term infant as one who is greater than 37 weeks’ gestation. Recent evidence, however, has demonstrated that infants born at 37 weeks’ gestation behave differently from infants delivered at 39 and 40 weeks’ gestation. The more mature term infant (39 or 40 weeks) has fewer respiratory problems, less difficulty with feeding and hyperbilirubinemia, reduced birth injury, a greater ability to respond to infection, and an overall reduction in rates of neonatal complications.
Given that infants born before 37 weeks have even greater liability for problems, the recognition that true term status begins at about 39 weeks’ gestation has led the American College of Obstetrics and Gynecology (ACOG) and the American Academy of Pediatrics (AAP) to recommend that no infants be delivered electively before 39 weeks. ∗†
2. What is the average birth weight of a term infant?
The mean birth weight of a term infant is approximately 3400 grams, or approximately 7 pounds, 7 ½ ounces. Mean length, which is sometimes difficult to measure accurately, is approximately 52 to 53 centimeters, or 20 inches, and head circumference averages 34 centimeters, or approximately 13.5 inches. Of note is the fact that birth weight in recent years has declined slightly, even though premature births have been declining. ∗
3. How often is neonatal resuscitation necessary for a term infant?
Approximately 10% of all infants need some assistance at birth (e.g., stimulation, oxygen), and approximately 1% need extensive assistance (e.g., positive pressure ventilation, fluids, drugs) at the time of birth. ∗
4. What are the critical skills needed by any individual called upon to resuscitate a neonate?

5. What is an Apgar Score?
The Apgar score is a clinical assessment developed by Dr. Virginia Apgar at Columbia University during the early 1950s. Dr. Apgar was a great pioneer for women in medicine, and her development of the Apgar score is just one of her many landmark contributions to medicine. Although she was an anesthesiologist, she was very concerned about the status of newborn infants immediately after delivery. Her score, which was designed to evaluate both the immediate and long-term well-being of a neonate, has been reassessed periodically and still appears to be as valid today as when it was first introduced.
The Apgar score is determined at 1 and 5 minutes of life and consists of the measures listed in Table 1-1. These measures are scored 0, 1, or 2, then totaled.
TABLE 1-1
THE APGAR SCORE
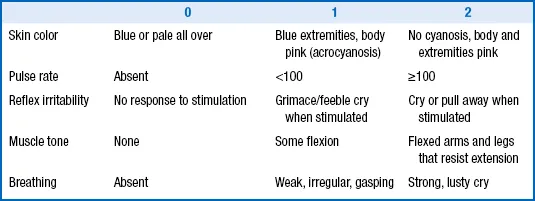
It is rare for an infant to have an Apgar score of 10 (the highest possible score) in the absence of oxygen administration because the exposure of most newborn infants to the environmental temperature of the delivery room will cause some acrocyanosis of the hands and feet, reducing the potential score to 9. An Apgar score above 7 is considered good, one between 4 and 7 demands close observation, and one that is 3 or lower usually requires some intervention. Even with the changes that have occurred in modern medicine, the Apgar score has retained its value. ∗
5a. How should the Apgar change in the immediate postnatal period?
One of the other important aspects of the Apgar score is the change between 1 and 5 minutes of life. For vigorous term infants the Apgar score does not change significantly between 1 and 5 minutes of life. Changes in the Apgar score, however, are useful for assessing the response to resuscitation. For example, a newborn infant who has a 1-minute Apgar score of 3 and a 5-minute score of 8 has probably had some terminal difficulty at the time of delivery that has been quickly surmounted. On the other hand, the neonate with Apgar scores of 3 and 4 at 1 and 5 minutes is not responding well and may need further intervention. When an infant’s 5-minute score is 5 or lower, it has become customary to continue to provide Apgar scores every 5 minutes up to 20 minutes of life or until the score is above 7. Slow improvement in an Apgar score may be associated with some element of hypoxia or ischemia during the delivery, but there are many other reasons for low Apgar scores. A low Apgar score at 1 or 5 minutes has a poor positive predictive accuracy for later disabilities.
6. What should be done to prepare for the delivery of a term infant?
When called to the delivery of a term infant, the clinician should first make sure that all possible tools that might be needed for resuscitation and maintenance of a thermal neutral environment are ready. Although the great majority of term infants in an uncomplicated pregnancy do not require any intervention, it is important to be prepared for any possibility. In addition, a number of other routine items are necessary. On arrival in the delivery room the following items should be checked:
7. Why is temperature control of the delivery room so important for a term infant?
Immediately before delivery the fetus is bathed in amniotic fluid and maintained at a temperature identical to that of the mother. Within se...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Contributors
- Preface to the Third Edition
- Preface to the First Edition
- Acknowledgments
- Top 100 Secrets
- Chapter 1: Care of the Term Infant
- Chapter 2: Fetal Growth and Development
- Chapter 3: Obstetric Issues, Labor, and Delivery
- Chapter 4: Family-Centered and Developmental Care in the Neonatal Intensive Care Unit
- Chapter 5: NICU Environment and Principles of Infection Control
- Chapter 6: Cardiology Secrets
- Chapter 7: Dermatology
- Chapter 8: Endocrinology and Metabolism
- Chapter 9: Fluid, Electrolyte, Acid–Base, and Renal-Developmental Physiology and Disorders
- Chapter 10: Gastroenterology and Nutrition
- Chapter 11: Genetics
- Chapter 12: Hematology and Transfusion Medicine
- Chapter 13: Infection and Immunity
- Chapter 14: Neurology
- Chapter 15: Neonatal Ophthalmology
- Chapter 16: Orthopedics
- Chapter 17: Pain Management in the Neonate
- Chapter 18: Pulmonology
- Chapter 19: Surgery
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Fetal & Neonatal Secrets by Richard Polin,Alan R. Spitzer,Richard A. Polin in PDF and/or ePUB format, as well as other popular books in Médecine & Gynécologie, obstétrique et profession de sage-femme. We have over 1.5 million books available in our catalogue for you to explore.