Get a quick, expert overview of the many key facets of obesity management with this concise, practical resource by Dr. Jolanta Weaver. Ideal for any health care professional who cares for patients with a weight problem. This easy-to-read reference addresses a wide range of topics – including advice on how to "unpack" the behavioral causes of obesity in order to facilitate change, manage effective communication with patients suffering with weight problems and future directions in obesity medicine.- Features a wealth of information on obesity, including hormones and weight problems, co-morbidities in obesity, genetics and the onset of obesity, behavioral aspects and psychosocial approaches to obesity management, energy and metabolism management, and more.- Discusses pharmacotherapies and surgical approaches to obesity.- Consolidates today's available information and guidance in this timely area into one convenient resource.
- 350 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Practical Guide to Obesity Medicine
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MédecineSubtopic
Endocrinologie et métabolismePart I
The Size of the Problem
Chapter 1
The Global Problem of Obesity
Dr. Susan E. Jones, MB, CHB, MD, FRCP
Abstract
The incidence and prevalence of obesity is continuing to rise throughout the world, which is resulting in higher rates of conditions such as type 2 diabetes, cardiovascular disease, and cancer. This chapter outlines the epidemiology of obesity and discusses the challenges in interpreting obesity data on a global scale. The economic costs of obesity are discussed with particular reference to developing nations that are becoming increasingly urbanized. The role of childhood obesity in countries where low birthweight (LBW) is common is also discussed. The epidemiologic data from the INDIAB study are also summarized as these contextualize the problems of obesity and LBW with respect to diabetes and hypertension.
Keywords
BMI; Diabetes; Epidemiology; Obesity; SE Asia; Waist circumference
Introduction
Obesity increases the risk of a wide range of medical conditions including type 2 diabetes, cardiovascular disease, and all cancers, with the exception of pancreatic, prostate, and esophageal cancers (females).1 Obesity costs the UK’s National Health Service in excess of £5.1 billion per annum, and this figure is set to rise because the prevalence of the condition increases year on year.2 The prevalence of obesity in the United Kingdom has nearly doubled between the years 1993 and 2011. Obesity rates in males rose from 13% to 24% and in females from 16% to 26%.3 Total societal and economic burden of obesity and overweight in the United Kingdom was estimated at £16 billion per annum in 2007 (1% of GDP) and this is predicted to rise to £50 billion by 2050 if the prevalence of obesity continues to increase at the same rate.3 Prevalence and economic data from the United Kingdom provide a “snapshot” of trends within Western healthcare systems but cannot be extrapolated widely because of a number of factors. Obesity is not just a “Western problem,” and there are many confounding variables that need to be addressed. “Developed” nations invariably have a very robust dataset for their healthcare, and obesity rates in the West are relatively easy to find; therefore data can be correlated to look at the effect of obesity on chronic health conditions.
Worldwide, the data collection methods are less robust, but this chapter aims to give an overview of how obesity is a truly global problem that is increasing year on year. The World Health Organization (WHO) and United Nations (UN) data are a major source of information on a wide range of noncommunicable diseases (NCDs) and also provide data on obesity. Closer analysis of these data shows a wide range of methodologies over the years, but data from India provide a modern perspective on the current state of obesity, which can be extrapolated more easily to less well developed countries, and are used throughout this chapter.
Definition of Obesity
WHO has classified obesity by body mass index (BMI),4,5 but this classification is controversial. BMI is calculated by an individual’s weight in kilograms divided by their height in meter squared and expressed as kg/m2. The original calculation was devised by a Belgian statistician, Adolphe Quetelet, in 1832. His remit was to study growth of “normal” men and to produce an index of relative weight to predict growth, which became known as the “Quetelet index.” From the outset he did not want to study obesity, but WHO adopted the index in 1995 to do just that4 and renamed it BMI. BMI was ever validated only in Caucasian males and not immediately transferrable to females or non-Caucasians.
BMI takes no account of the distribution of body fat6 and is a “blunt instrument” to identify individuals at risk of morbidity due to their weight. Waist circumference measurement can be used as a screening tool to identify individuals at risk of increased visceral fat deposition, which is an independent risk factor for cardiovascular disease and type 2 diabetes.7–9 To identify “pathologic obesity,” one, therefore, needs both waist circumference and BMI, but these data are not always available together; therefore BMI continues to be used as the main indicator of obesity.
Both BMI and waist circumference have been validated in Caucasian populations, but it is widely recognized that Southeast Asian (SE Asian) populations are different. SE Asians have higher rates of metabolic syndrome and type 2 diabetes than their age, BMI, and waist circumference matched Caucasian counterparts in the same environment.10 This observation has been previously noted and led to redefinition of obesity among SE Asian population.11–13 Table 1.1 shows classification of obesity between Caucasian and SE Asians and emphasizes how obesity rates can be underestimated among SE Asians if BMI standards for Caucasians are applied to them.
Obesity Rates Worldwide
WHO produces regular reports on a wide range of health issues among which are the NCDs that include, among others, diabetes and cardiovascular disease. The Global Health Observatory (GHO) data on NCD include rates of overweight and obesity based on BMI, but waist circumference data are not available. In 2014 GHO estimated that 39% adults aged 18 years and above were overweight and 13% were obese, and the mean BMI of the world’s population was 24 kg/m2.14 It must be appreciated that these data are only estimates and as such can map trends in obesity by geographic region but cannot provide true prevalence data. Countries around the world report voluntarily to WHO on their NCD prevalence and WHO used a “standard year” of 2010 to provide baseline data. The figures produced are based on published and unpublished literature with a variety of statistical tests, including regression analysis, to produce the final data.15 The data for countries with “developed” healthcare systems who publish epidemiologic and other research are likely to be very robust and the estimated rates are fairly accurate. In contrast, “developing” nations in whom NCD research and healthcare systems are not yet at the same level as Western nations will, by definition, have underestimation of obesity rates.
Table 1.1
Body Mass Index (BMI) Classification for Caucasians and Southeast (SE) Asians
| BMI kg/m2 | ||
| Caucasian | SE Asian | |
| Underweight | <18.5 | <18.5 |
| Normal | 18.5–24.9 | 18.5–22.9 |
| Overweight | 25.0–29.9 | 23.0–24.9 |
| Obese I | 30.0–34.9 | 25.0–29.9 |
| Obese II | 35.0–39.9 | ≥30.0 |
| Obese III | ≥40.0 | |
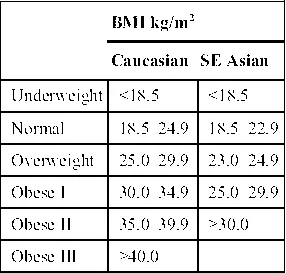
Data from WHO. Obesity: preventing and managing the global epidemic. Report of a WHO Expert Consultation. WHO Technical Report Series 89, Geneva: World Health Organisation; 2000, WHO/IASO/IOTF. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Melbourne: Health Communications Australia; 2000, and WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004:157–163.
To produce its reports WHO divides the world into regions that have vastly different healthcare resources ...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- List of Contributors
- Preface: Does “Benign Obesity” Exist?
- Part I. The Size of the Problem
- Part II. Hormones and Weight Problems
- Part III. Co-Morbidities in Obesity
- Part IV. Genetics and Onset of Obesity
- Part V. Bevioural Aspects and Psychosocial Approach to Obesity Management
- Part VI. Energy and Metabolism Management
- Part VII. Pharmacotherapies in Obesity
- Part VIII. Surgical Approach
- Part IX. Bottom Line
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Practical Guide to Obesity Medicine by Jolanta Weaver in PDF and/or ePUB format, as well as other popular books in Médecine & Endocrinologie et métabolisme. We have over 1.5 million books available in our catalogue for you to explore.