The ability to effectively assess cognitive and other behavioral functions is an essential skill for neurologists, psychiatrists, geriatricians, nurses, and other clinicians who perform clinic and bedside examinations. Unique in the field, The Mental Status Examination Handbook is a user-friendly, comprehensive resource that provides practical guidance on cognitive assessment, clarifies mental status testing procedures, and assists with decision making for neuropsychological referrals. This detailed manual draws from the full history of behavioral neurology testing, making the complex and challenging area of cognitive assessment accessible for both students and practitioners.- Offers guidance on how to choose and perform a large number of mental status tests, with information on selected test materials and normative values.- Covers the bedside evaluation of arousal, attention, memory, language, perception, executive abilities, and other cognitive and behavioral areas.- Provides an authoritative assessment and compendium of commonly used mental status scales, inventories and questionnaires.- Describes relevant correlations with formal neuropsychological testing, neuroimaging, and neuropsychiatric disease.- Explains how to weigh, use, and understand mental status scales and neuropsychological instruments.- Discusses the meaning of cognitive symptoms and signs, and their neuroanatomical and neuropathological correlations.
- 320 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Mental Status Examination Handbook E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Section II
Mental Status Testing
Chapter 5
Overview of the Mental Status Examination
The mental status examination (MSX) employs a cognitive domain approach, examining fundamental aspects, such as arousal and attention, and instrumental aspects, such as language, memory, perception, and executive abilities. The mental status examiner often starts with a more limited screening procedure, either a brief MSX, mental status scales, or a targeted MSX, which can be composed of isolated parts of the neurobehavioral status examination (NBSE). Here we will expand on the brief MSX and outline the major elements of the NBSE.
Brief MSX
For most clinical encounters, either in-person or by telemedicine, the clinician may quickly probe wide areas of the patient's cognition with a brief MSX. This has the advantage of being able to assess critical cognitive domains in 5 minutes or less; clinicians can quickly examine one or two representative tasks in awareness, orientation, attention, language, memory, and perception (Table 5.1). The subsequent NBSE sections discuss these cognitive domains in greater detail.
TABLE 5.1
| Awareness | Observation for awareness; if necessary, loudly call name, sternal pressure, pinch Achilles tendon. |
| Orientation | What is the date (day, month, year, day of week, time)? Where are we; the name of this place, city, state, floor/location? |
| Attention | Digit span forward (until misses two trials at a level); If necessary, subtraction by 7s from 100 (or by 3s from 20). |
| Language | Naming of six common items in the room or pictures/drawings; if necessary, ask for as many names of animals in a 1 minute. |
| Memory | Give three to four unrelated words for subsequent recall in 1 or more minutes; (during delay period, can ask for three recent or current events). |
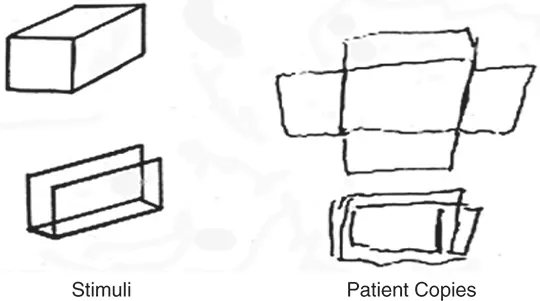
| Perception | Copy a three-dimensional “Necker” cube; if necessary, add two-dimensional drawing (e.g., intersecting pentagons). |
Step 1: Awareness. The brief MSX starts with deliberate observation of the patient's general behavior with the most prominent focus on determining their state of alertness and wakefulness. Although most patients requiring mental status testing are sufficiently aware and awake, occasionally there is evidence of disturbances of arousal, such as lethargy, drowsiness, sleepiness, stupor, and coma. In situations in which the patient lacks significant awareness, the examiner can check for arousal with verbal stimulation (loudly calling their name) or applying mild physical discomfort (sternal pressure, pinching the Achilles tendon).
Step 2: Orientation. The examiner asks the patient to state the current date and place. Orientation in the clinical setting is a sensitive general measure of awareness, attention, and memory. In the absence of a watch or other obvious display of the time, the patient's knowledge of the exact time of day can be a further extension of the assessment for temporal orientation. For place, asking about their floor or location in the building is of additional value.
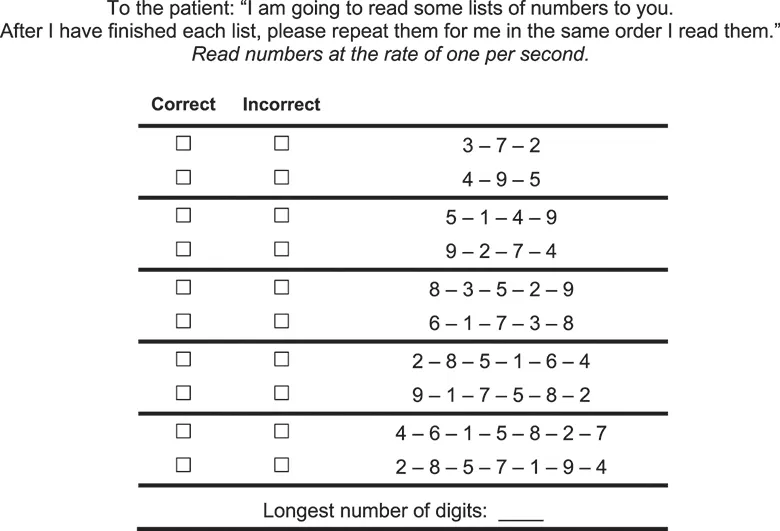
Step 3: Attention. Proficiency in attention is a prerequisite for adequate performance in instrumental abilities, such as memory and perception. The examiner most commonly screens the patient's ability to maintain attention with a digit span. Random digits are given, one per second, starting with three (Fig. 5.1). The patient is asked to recite them back in the same order. Two trials are given at each ascending level until the patient misses both trials. His/her digit span is the level just before missing both trials. If necessary, the examiner can do other serial recitation tasks that include subtracting from 100 by 7s (or the easier version of subtracting from 20 by 3s).
Step 4: Language. Most MSX depends on understanding verbal commands and the ability to give verbal responses. Abnormal language function (aphasia) can therefore compromise subsequent aspects of the MSE. Two subtests—naming ability and word-list generation (verbal fluency)—are particularly sensitive to language disturbances and act as good screening tests. First, ask the patient to name six common items pointed out in the room or as pictures/drawing. If more language information is desired, have the patient generate the names of as many animals as he or she can in 1 minute, with the expectation of generating at least 12.
Step 5: Memory. The examiner can screen declarative episodic memory through the patient's ability to recall a list of words. One easy test in the clinical setting is with a three to four word-learning task with a 1 or more minute delay before asking for their recall. To avoid continued rehearsal, the patient must do other cognitive tasks during this recall or “interference” period, such as recalling three current events in the news and performing the perception task from Step 8. One can also save the orientation questions for this interference period.
Step 6: Perception. Visuospatial skills depend on a number of areas of the brain, which can harbor perceptual deficits without demonstrable abnormality on other MSX tests. The ability to copy a three-dimensional cube drawing is a common visuospatial perceptual screening test (Fig. 5.2). Abnormalities can involve its three-dimensional perspective, the presence of parallel faces, the number of surfaces, and the placement of internal lines. The examiner can add two-dimensional drawings if the patient is quite impaired (e.g., copying intersecting pentagons).
Although a detailed evaluation is not necessary in all patients, a more extensive assessment is indicated if the brief MSX discloses problems or if the patient complains of ongoing cognitive difficulty. In this situation, the clinician may choose additional mental status tasks from the NBSE that offer information of value for a particular patient's deficits. Although this can also be performed through formal psychometric examinations, the clinician can obtain excellent information from the NBSE, and in many instances, this provides information unavailable from any laboratory study.
Overview of the NBSE
The following is an outline of the NBSE, which can take a few minutes to several hours to complete, depending on how much of it is done. It is organized into 14 “domains” (Table 5.2), which are much expanded with many more tests or tasks elaborated on in Chapters 6–14. This is not the only possible organization of the NBSE, but it is one method that has proven practical in terms of the hierarchical order of testing and the ability to localize dysfunction in the brain. The examiner can use elements of the NBSE for targeted MSX or can modify them for patients with visual or auditory impairment. The examiner needs to consider the patient's education, intellectual background, and facility with English before. Finally, the examiner must perform the NBSE as part of the overall neurological examination.
- 1. General Behavioral Observations. The experienced examiner begins with a thoughtful inspection of the patient's overt behavior and interactions with others and the environment. The patient's general behavior may be the only method of assessment available in a very uncooperative, agitated, or arousal-impaired patient. Yet, careful behavioral observations in and of themselves can provide a very informative mental status assessment. If the patient is sufficiently awake and aware, further consideration of his/her general behavior includes attention to the patient's appearance, attitude, and affect. For example, a slovenly appearance with poor personal hygiene can reflect dementia, psychosis, depression, apathy, and other behavioral disturbances. Specific findings such as neglect of one side of the body can indicate a focal hemispheric insult. Patients may be cooperative, indifferent, disinterested in the interview, or hostile. The examiner also considers their prevailing affect, whether it reflect...
Table of contents
- Cover Image
- Title Page
- Copyright
- Dedication
- Preface
- Table of Contents
- Section I Fundamentals of Mental Status Testing
- Section II Mental Status Testing
- Section III Scales or Inventories, Neuropsychological Tests, and Computerized Techniques
- Appendix A Index of Mental Status Tasks
- Appendix B Mental Status Scales
- Key Select References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Mental Status Examination Handbook E-Book by Mario F. Mendez in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.