With cases reflecting the classic presentation format of each disease process, this book prepares students for patient encounters during their oral and maxillofacial surgery rotations. It also helps residents learn and review "high yield" material that is commonly found in oral and maxillofacial training and on board examinations. It highlights clinical information that is commonly asked during rounds, in the operating room, and during examinations. For each case, it includes an overview of the most common clinical presentation, physical exam findings, diagnostic tools, complications, treatment, and a discussion of any controversial issues that may surround the case. The authors describe Clinical Review of Oral and Maxillofacial Surgery as "A little reach for the dental student, right on target for the OMS resident, and a strong refresher for OMS board certification." This title includes additional digital media when purchased in print format. For this digital book edition, media content is not included.- Case-based format prepares students and residents to pass the OMSSAT, with the Table of Contents corresponding to the exam's categories and questions.- 95 clinical cases focus on essential information regarding each disease process.- Detailed illustrations -- including radiographs and clinical photographs or drawings -- provide a visual guide to conditions, techniques, diagnoses, and key concepts.- Contributing authors include recent graduates or senior residents in oral and maxillofacial surgery, so they are fully cognizant of students' and residents' needs as they prepare for cases, exams, and surgical procedures.- Complements other Elsevier books such as Peterson: Contemporary Oral and Maxillofacial Surgery, Fonseca: Oral and Maxillofacial Surgery, and Ward Booth: Maxillofacial Surgery.
eBook - ePub
Clinical Review of Oral and Maxillofacial Surgery - E-Book
Clinical Review of Oral and Maxillofacial Surgery - E-Book
- 576 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinical Review of Oral and Maxillofacial Surgery - E-Book
Clinical Review of Oral and Maxillofacial Surgery - E-Book
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Oral Health & SurgeryChapter 1
Oral and Maxillofacial Radiology
This chapter addresses:
• Multilocular Radiolucent Lesion in the Pericoronal Region (Keratocystic Odontogenic Tumor [Odontogenic Keratocyst])
• Unilocular Radiolucent Lesion of the Mandible
• Multilocular Radiolucent Lesion in the Periapical Region (Ameloblastoma)
• Unilocular Radiolucent Lesion in a Periapical Region (Periapical Cyst)
• Mixed Radiolucent-Radiopaque Lesion (Ossifying Fibroma)
• Cone-Beam Computed Tomography (CBCT)
Interpretation of radiographs is a routine part of the daily practice of oral and maxillofacial surgery. Commonly obtained radiographs at the office include the periapical, occlusal, panoramic, and lateral cephalometric radiographs. Cone beam computed tomography (CBCT) scans are becoming more readily available in many offices. Although this technology is extremely useful, its indications, liabilities, and advantages have to be clearly recognized. As the future unfolds, the advancing technology will improve upon office imaging modalities that will facilitate diagnosis and treatment. Therefore, a knowledge of normal radiographic anatomy and clinical skill in recognizing pathologic conditions become even more essential.
Despite clinicians' ability to read and interpret many different imaging studies, the oral and maxillofacial radiologist will play an increasingly greater role in the practice of oral and maxillofacial surgeons.
This section includes the radiographic presentation of five important and representative pathologic processes, in addition to a new case demonstrating the use of CBCT. Included in each case is the differential diagnosis of associated conditions, to guide further study.
Figure 1-1 shows the most common location of several radiographically detectable maxillofacial pathologic processes.
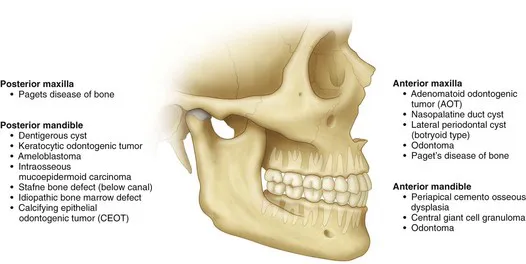
Figure 1-1 The most common location of several radiographically detectable maxillofacial pathologic processes.
Multilocular Radiolucent Lesion in the Pericoronal Region (Keratocystic Odontogenic Tumor [Odontogenic Keratocyst])
Piyushkumar P. Patel, Chris Jo and Shahrokh C. Bagheri
CC
A 20-year-old man is referred for evaluation of a swelling on his right mandible.
Keratocystic Odontogenic Tumor (KCOT)
Keratocystic odontogenic tumors (KCOTs) show a slight predilection for males and are predominantly found in individuals of Northern European descent. The peak incidence is seen between 11 and 40 years of age. Patients with larger lesions may present with pain secondary to infection of the cystic cavity. Smaller lesions are usually asymptomatic and are frequently diagnosed during routine radiographic examination.
The World Health Organization (WHO) has recommended the use of the term keratocystic odontogenic tumor (KCOT), rather than odontogenic keratocyst (OKC), because the former name better reflects the neoplastic behavior of the lesion. Genetically, the lesion shows a repeatable chromosomal abnormality (PTCH gene on chromosome 9q22.3-q31).
HPI
The patient complains of a 2-month history of progressive, nonpainful swelling of his right posterior mandible. (About 65% to 83% of KCOTs occur in the mandible, most often in the posterior body and ramus region. KCOTs account for approximately 3% to 14% of all oral cystic lesions.) The patient denies any history of pain in his right lower jaw, fever, purulence, or trismus. He does not report any neurosensory changes (which are generally not seen with KCOTs).
MHX/PDHX/Medications/Allergies/SH/FH
Noncontributory. There is no family history of similar presentations.
Nevoid basal cell carcinoma syndrome (NBCCS) is an autosomal dominant inherited condition with features that can include multiple basal cell carcinomas of the skin, multiple KCOTs, intracranial calcifications, and rib and vertebral anomalies. Many other anomalies have been reported with this syndrome (Box 1-1). The prevalence of NBCCS is estimated to be 1 in 57,000 to 1 in 164,000 persons.
Box 1-1
Diagnostic Criteria for Nevoid Basal Cell Carcinoma Syndrome
Examination
Maxillofacial. The patient has slight lower right facial swelling isolated to the lateral border of the mandible and not involving the area below the inferior border. The mass is hard, nonfluctuant, and nontender to palpation (large cysts may rupture and leak keratin into the surrounding tissue, provoking an intense inflammatory reaction that causes pain and swelling). There are no facial or trigeminal nerve deficits (paresthesia of the inferior alveolar nerve would be more indicative of a malignant process). The intercanthal distance is 33 mm (normal), and there is no evidence of frontal bossing. His occipitofrontal circumference is normal (an intercanthal distance [the distance between the two medial canthi of the palpebral fissures] of greater than 36 mm is indicative of hypertelorism, and an occipitofrontal circumference greater than 55 cm is indicative of frontal bossing; both can be seen with NBCCS).
Neck. There are no palpable masses and no cervical or submandibular lymphadenopathy. Positive lymph nodes would be indicative of an infectious or a neoplastic process. A careful neck examination is paramount in the evaluation of any head and neck pathology.
Intraoral. Occlusion is stable and reproducible. The right mandibular third molar appears to be distoangularly impacted (KCOTs do not typically alter the occlusion). The interincisal opening is within normal limits. There is buccal expansion of the right mandible, extending from the right mandibular first molar area posteriorly toward the ascending ramus. Resorption of bone may include the cortex at the inferior border of the mandible, but this is observed at a slower rate than in intermedullary bone, which is less dense. For this reason, KCOTs characteristically extend anteroposteriorly than buccolingually. This pattern of expansion into less-dense bone explains why maxillary KCOTs show more buccal than palatal expansion and often expand into the maxillary sinus. There is no palpable thrill or audible bruit, both of which are seen with arteriovenous malformations. The oral mucosa is normal in appearance with no signs of acute inflammatory processes.
Thorax-abdomen-extremity. The patient has no findings suggestive of NBCCS (e.g., pectus excavatum, rib abnormalities, palmar or plantar pitting, and skin lesions; see Box 1-1).
Imaging
A panoramic radiograph is the initial screening examination of choice for patients presenting for evaluation of intraosseous mandibular pathology (10% to 20% of KCOTs are incidental radiographic findings). This provides an excellent overview of the bony architecture of the maxilla, mandible, and associated structures. CT scans can be obtained when large lesions are found. CT scans are valuable in that they provide additional information, such as the proximity of adjacent structures (e.g., the mandibular canal), the integrity of cortical plates, and the presence of perforations into adjacent soft tissues. CT scans provide accurate assessment of the size of the lesion and can demonstrate additional anatomic details (or lesions) that do not appear on panoramic radiographs.
A CBCT scan is appropriate for the evaluation of this lesion. Given its higher resolution, lower radiation dose (approximately 20% of the radiation of a conventional [helical] CT ), and lower cost, a CBCT can replace helical CT for evaluation and follow up of such a lesion. The CBCT scan can also be used to create a stereolithic model of the area of interest.
It has been demonstrated that T2-weighted magnetic resonance imaging (MRI) can detect KCOTs in 85% of new cases with a readily recognizable pattern. However, the use of MRI for management of suspected OKCs is not routine.
In this patient, the panoramic radiograph reveals a large, multilocular radiolucent lesion with possible displacement of the right mandibular third molar (Figure 1-2). T...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Acknowledgments
- Chapter Editors and Contributors
- Foreword
- Preface
- Chapter 1: Oral and Maxillofacial Radiology
- Chapter 2: Pharmacology
- Chapter 3: Anesthesia
- Chapter 4: Oral and Maxillofacial Infections
- Chapter 5: Dentoalveolar Surgery
- Chapter 6: Dental Implant Surgery
- Chapter 7: Head and Neck Pathology
- Chapter 8: Craniomaxillofacial Trauma Surgery
- Chapter 9: Orthognathic Surgery
- Chapter 10: Temporomandibular Joint Disorders
- Chapter 11: Oral Cancer
- Chapter 12: Reconstructive Oral and Maxillofacial Surgery
- Chapter 13: Facial Cosmetic Surgery
- Chapter 14: Syndromes of the Head and Neck
- Chapter 15: Medical Conditions
- Appendix 1: Abbreviations
- Appendix 2: Normal Laboratory Test References for Adults
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Review of Oral and Maxillofacial Surgery - E-Book by Shahrokh C. Bagheri,Chris Jo in PDF and/or ePUB format, as well as other popular books in Medicine & Oral Health & Surgery. We have over 1.5 million books available in our catalogue for you to explore.