Traumatic experiences are distressingly common, and the risks of developing posttraumatic stress disorder are high. But in recent years the field of traumatology has grown strong, giving survivors and their counselors firmer footing than ever before to seek healing. This book is a combined effort to introduce counseling approaches, trauma information, and Christian reflections to respond to the intense suffering people face.With extensive experience treating complex trauma, Heather Gingrich and Fred Gingrich have brought together key essays representing the latest psychological research on trauma from a Christian integration perspective.Students, instructors, clinicians, and researchers alike will find the following:
An overview of the kinds of traumatic experiences.
Coverage of treatment methods, especially those that incorporate spirituality.
Material to critically analyze as well as emotionally engage trauma.
Theoretical bases for trauma treatment and interventions.
References for further consideration and empirical research.
Christian Association for Psychological Studies (CAPS) Books explore how Christianity relates to mental health and behavioral sciences including psychology, counseling, social work, and marriage and family therapy in order to equip Christian clinicians to support the well-being of their clients.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
THE CRUCIAL ROLE OF CHRISTIAN COUNSELING APPROACHES IN TRAUMA COUNSELING
FRED C. GINGRICH AND HEATHER DAVEDIUK GINGRICH
For he has not despised or scorned the suffering of the afflicted one; he has not hidden his face from him but has listened to his cry for help.
PSALM 22:24
So many are deeply wounded as a result of the trauma they have experienced. How can we even begin to meet the need? Where do we start? What do secular approaches have to offer, and where do they fall short? How are we as Christian counselors in a unique position to journey with survivors?
We have no definitive answers to these and similar questions. We will attempt, however, to address some overarching topics that we hope will give you a framework from which to approach your reading of the chapters that follow.
In this chapter we begin by addressing the question of the goal of trauma treatment. We go on to examine a specific model of trauma recovery, the 4-D model (Frewen & Lanius, 2015), describing and evaluating it. We then suggest that an expanded version of this model addresses some of its shortfalls. Our intention is to provide you with an idea of what recovery looks like, which will influence how you view further discussions on treatment as you read various chapters in this book.
The next section of the chapter looks at the area of research with respect to evidence-based practice for trauma treatments (EBTTs). It serves as an overview of the terminology and issues surrounding EBTTs and directs readers to helpful resources on the topic.
We then turn our attention to ethical issues surrounding trauma treatment and introduce the area of trauma and spirituality. Finally, we make some brief comments about the need for additional and ongoing effort to wrestle with our theology of suffering—the crux of what we as Christians have to offer.
What Is the Goal of Trauma Treatment?
The various chapters of this book imply a variety of ways of conceptualizing trauma and present a multitude of treatment approaches to trauma. Of course, to some degree the choice of trauma treatment utilized depends on the particular population, the background of the treatment provider, and a number of contextual factors. Obviously, treatment will be different if the client is a recent victim of a natural disaster rather than a sexual-abuse survivor of long-term, complex interpersonal trauma. Regardless of the type of trauma, though, the ultimate goal is healing.
But what are the hallmarks of healing? Is a decrease in posttraumatic symptoms such as intrusive reexperiencing in the form of flashbacks or nightmares what we mean by healing? Or is healing more than symptom reduction? Do trauma survivors need to have wrestled personally with the existential/spiritual questions related to how to make meaning out of suffering in order to be considered healed? But then again, none of us will be fully whole, that is, fully healed, this side of eternity. So perhaps the often-used metaphor of healing as a journey, a process, rather than as an end goal, would be most helpful when thinking about therapeutic work with trauma survivors. Successful termination of therapy, then, would come at the point in the journey at which the client determines they are healed “enough” for at least the time being.
A Model of Trauma Recovery: The 4-D Model
In our perusal of the literature, our attention was drawn to the 4-D model of a victim’s sense of self as it relates to trauma and recovery (Frewen & Lanius, 2015). While not the only or necessarily even the best model of trauma therapy, it offers a clinically helpful conceptual framework to which we have added additional theoretical constructs including spirituality.
Description of the model. The model suggests that there is, ideally, movement happening for the client from a sense of identity emerging from a traumatized self to an identity of a recovered self. This movement fits with the idea of trauma healing as a journey that we alluded to above; it is a process, and our goal as clients and clinicians is to see some progression toward healing, although the movement may be quite different depending on numerous factors such as type of trauma, severity, and pretrauma adjustment.
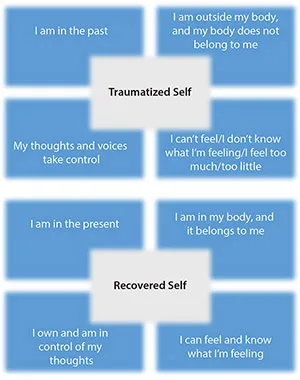
The original four dimensions of the Frewen and Lanius (2015) model refer to time, body, thought, and emotion. Figure 1.1 illustrates the original model.
Figure 1.1. 4-D model sense of self from trauma to recovery (Frewen & Lanius, 2015, p. 304)
The dimensions and descriptions of movement from a sense of traumatized self to a sense of recovered self are as follows:
Time. I am fixated/focused on the past—the trauma—and I am moving toward becoming more focused in the present.
Body. At times I feel outside my body, that my body does not belong to me, and that things happened to my body, and I am moving toward a clearer sense of being my body and that it belongs to me, that my identity and body are integrated (cf. Levine, 2010, 2015; van der Kolk, 2015).
Thought. Thoughts and voices or messages are intrusive and take control, and I am moving toward a sense of owning and being in control of my thoughts.
Emotion. Either I can’t feel anything, I don’t know what I’m feeling, or I feel too much, and I am moving toward being able to feel and knowing what I’m feeling, and it is not overwhelming me.
Questions that arise from the model. We believe that these dimensions are a helpful starting place from which to assess trauma and healing from trauma. However, some questions arise from looking at these dimensions more carefully. Consider the following:
To what degree does inclusion of the body as one of the four dimensions make sense? To begin with, the brain and nervous system are crucial parts of the body that recent research findings have shown to be deeply affected by trauma (see chap. 3). Additionally, if we are to be true to a biopsychosocial model of the person (McRay, Yarhouse, & Butman, 2016), we must take seriously the physically disorienting dimension of trauma in terms of somatoform symptoms, and even where the body is in place and time (i.e., with respect to symptoms of depersonalization and intrusive reexperiencing of physical symptoms that can be part of flashbacks). Trauma tends to disintegrate this biopsychospiritual connection, resulting in dissociated aspects of a sense of self and experience (Gingrich, 2013). Also, a strong argument can be made for a biblical anthropology that rests on our being created as an embodied, unified body-soul-spirit (Benner, 1998). Jesus’ resurrection and ascension as an embodied person affirms that the body is essential to our existence. His body was tortured, and even after the resurrection he carried the signs in his body. Of course, the dimensions of thought and emotion are also essential to a biblical anthropology and to our understanding of what trauma destroys and what mental health in God’s image looks like.
To what degree does the movement from trauma to recovery involve an increased sense of an integrated self and individual identity, as well as identity within or as part of a group (e.g., familial, ethnic, religious)? We briefly looked at the separation of the physical sense of self from the other aspects of self in the discussion of the body in the bullet point above. We also alluded to disintegration of the psychological and spiritual aspects of self. However, the relational dimension of identity that is central in more group-oriented cultures is not addressed by the model. The broader sociopolitical and economic contexts of trauma also are often vastly underacknowledged. This would be particularly evident in disasters, war, and other mass casualty contexts.
The dimensions of the model, considered in combination, point to some of the complexity of trauma symptoms. But the model does not take into account the differences in severity and life disruption that individuals may experience in response to trauma. Since behavioral symptoms are often most readily observed by others, what does a reduction in symptoms in the other dimensions look like? Change in behavioral symptoms such as compulsive, avoidant, or dissociated behavior, for example, are more easily seen, yet some of the emotional distress may actually be more disturbing for the client.
Meaning making is a key component of the trauma healing process. This has been emphasized in Park’s research (e.g., 2013; Slattery & Park, 2015). Has the survivor been able to make meaning of the suffering? How will the survivor’s future be affected? What is the role of hope, and how do our current circumstances interact with the future trajectory of God’s involvement with humanity (i.e., our “blessed hope,” Titus 2:13; see also 1 Thess 4:13-18)?
What is the place of spirituality in the emergence, continuity, and healing of the self? How crucial is it? How does it operate to facilitate healing? Where is God in the midst of the trauma narratives people tell? From our perspective, a model of trauma must consider spirituality as it interacts with all dimensions. For instance, with respect to the dimension of time, we suggest that faith, and particularly a biblical perspective, includes extensive attention to the history of God working in and through difficult situations over time. We believe, therefore, that whichever trauma model we adopt, we should consider spirituality as a key element of what is negatively affected as a result of trauma, along with taking into account the role of spirituality in how trauma negatively affects the whole person and the community and how healing from traumatic experiences can occur.
Is the ultimate goal simply a recovered self, or is there something more that our spirituality has to offer? Specifically, while the literature (see appendix) refers extensively to coping, resilience, and posttraumatic growth, Christian faith provides hope that the biblical concept of shalom is a real possibility. Referring to biblical passages such as Isaiah 2:2-3 and 11:6-9, Wolterstorff (2013) argues that shalom, often translated as “peace,” is a much richer concept: “But Shalom goes beyond peace, beyond the absence of hostility. Shalom is not just peace but flourishing, flourishing in all dimensions of our existence—in our relation to God, in our relation to our fellow human beings, in our relation to ourselves, in our relation to creation in general” (p. 114). Flourishing is more than basic recovery from trauma—it is the essence of what our Christian faith has to offer (see chap. 2 in this volume for a further discussion of this dimension).
Our Expanded Model of Trauma Recovery: A Multidimensional Model
While no model can encompass all possible dimensions, we think that by adding the dimensions of behavior, relationships, identity, and spirituality, as well as the recovery aspects of coping, resilience, posttraumatic growth, and flourishing, the model is made more robust. Descriptions of these additional dimensions follow:
Behavior. I don’t always understand why I act the way I do, and I feel as though I don’t have control over my actions, and I am moving toward having a better understanding of and sense of control over my actions.
Relationships. I don’t have healthy relationships; either I don’t feel close to anyone and so experience emotional distance, or I feel swallowed up by the other person, or I’m terrified of being abandoned, or I feel continually victimized, and I am moving toward feeling connected without fear of abandonment or need to distance.
Spirituality. I have no sense of purpose in my suffering; if God is even a consideration, either I don’t believe in God or I believe in a God who is judgmental and punitive, and I am moving toward a sense of meaning that has resulted from my trauma; if I have a sense of relationship with God, there is more of a sense of connectedness to God without fear of reprisal.
Coping, resilience, posttraumatic growth, and flourishing. My life is overwhelmingly negative, and I am moving toward finding healthy ways to cope, discovering strengths and capacities for resilience, actually growing as a result of the trauma, and even flourishing in life.
Identity. My sense of self is diffuse; I don’t feel as though I am an integrated whole, and I am moving toward having a sense of myself as an integrated whole; I know who I am.
Evidence-Based Trauma Treatments (EBTTS)
As counselors we are ultimately interested in the arrow in figure 1.2. What can help us to help others move from a traumatized self to a recovered self? Below the arrow we have included three concepts that occur frequently in the trauma treatment literature, specifically coping, resilience, and posttraumatic growth. There are obvious overlaps in the definitions and treatment implications of these concepts, as can be readily seen by perusing...
Table of contents
Cover
Title Page
Contents
INTRODUCTION
PART ONE - FOUNDATIONAL PERSPECTIVES ON TRAUMA
PART TWO - INTERPERSONAL CONTEXTS OF TRAUMA
PART THREE - COMPLEX TRAUMA AND DISSOCIATION
PART FOUR - GLOBAL CONTEXTS OF TRAUMA
PART FIVE - CONCLUSION AND APPENDIX
APPENDIX: Religion, Spirituality, and Trauma: An Annotated Bibliography
Contributors
Subject Index
Praise for Treating Trauma In Christian Counseling
About the Editors
More Titles from InterVarsity Press
Copyright
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Treating Trauma in Christian Counseling by Heather Davediuk Gingrich, Fred C. Gingrich, Heather Davediuk Gingrich,Fred C. Gingrich in PDF and/or ePUB format, as well as other popular books in Psychology & Post-Traumatic Stress Disorder (PTSD). We have over 1.5 million books available in our catalogue for you to explore.