This volume presents pedagogical content to understand theoretical and practical aspects of diagnostic imaging techniques. It provides insights to current practices, and also discusses specific practical features like radiation exposure, radiation sensitivity, signal penetration, tissue interaction, and signal confinement with reference to individual imaging techniques. It also covers relatively less common imaging methods in addition to the established ones. It serves as a reference for researchers and students working in the field of medical, biomedical science, physics, and instrumentation.
Key Features • Focusses on the clinical applications while ensuring a steady understanding of the underlying science • Follows a bottom-up approach to cover the theory, calculations, and modalities to aid students and researchers in biomedical imaging, radiology and instrumentation • Covers unique concepts of nanoparticle applications along with ethical issues in medical imaging
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1 Diagnostic Medical Imaging Services with Myriads of Ethical Dilemmas in a Contemporary Healthcare ContextIs Artificial Intelligence the Solution?
Chandra Rekha Makanjee
DOI: 10.1201/9781003112068-1
Introduction
The Distributed Nature of Medical Imaging Services
The Complex Medical Imaging Encounter and Associated Complexities
Introducing AI in the DMI Context
The Basics of DMIE Ethical Principles
Multifaceted DMI Service Utilization Issues and Safety
Medical Imaging Contrast Agent Considerations and Safety Issues
Medical Imaging Errors and Safe Practice Culture
Issues of Occupational Exposure and Safe Practice
In the Best Interest of the Patients
Strategies to Consider in Dealing with the Myriads of Dilemma
Training Issues within the Medical Profession and DMI
Conclusion
References
Introduction
Modern diagnostic medical imaging (DMI) is complex, with access to multiple digital imaging modalities and techniques available. DMI methods supported by digital general radiographic and fluoroscopy systems, high-sensitivity detectors with quantum detection, advanced algorithms eliminating motion artefacts, and medical imaging monitors with a resolution of three to eight megapixels significantly differ from conventional screen film radiographic methods. Then current innovative technological advancement in computed tomography (CT), magnetic resonance imaging (MRI), isotopic methods, ultrasonography using elastography, and new solutions in doppler imaging are focused on reducing radiation exposure with better imaging capabilities and throughput (1).
This evolution reflects the utilization of complex ionizing and non-ionizing DMI technologies simultaneously, resulting in a constant flux in the diagnostic medical imaging healthcare professionals’ (DMIHCP) roles and responsibilities. This is mediated through technology including the social, biomedical, and psychological context, influenced by advances in the fields of physics, medicine, biology, and engineering and including innovations in computer and data sciences (2). This means working with a diverse range of medical and non-medical healthcare professionals (HCP) in achieving and ensuring equitable access to a timely diagnosis and quality outcomes for the person as the patient. In an artificial intelligence (AI) context, this can be achieved by using smart data analytics in patient scheduling, decision support for safe and appropriate order entry, natural language processing-based querying and annotation of radiology reports, resource utilization dashboards, and the prediction of healthcare economic trends. With neural networks capable of self-learning, constant and autonomous improvement and refinement of workflows can take place in the background. So, there is a shift in tasks that can yield larger net efficiencies, rather than mere pixel-based computer-aided detection tools (3).
From a healthcare systems perspective the DMIHCPs’ functioning extends well beyond the recognition of pathological patterns in images. DMIHCPs routinely employ “real” intelligence to convert accurate image interpretation into actionable, holistic patient-centric decision-making in variable medical settings ranging from office-based outpatient private imaging centres to tertiary academic research hospitals with a complex case mix and comorbid patients whose care as already mentioned involves multidisciplinary team consultations and involvement in problem solving. Further DMI services are distributed across various level of healthcare systems consisting of engineers, non medical and medical healthcare providers, physicists, technological specialist hence inherently interdependent in nature to achieve a seamless quality health outcomes.
An integral component of the aforementioned is the ethical aspect. Professional ethics is the basis for each professional’s work, as it includes values and principles, together with rights and duties that guide and support professionals (4). As stated earlier, DMI is inherently interdependent with a diverse range of HCPs both medical and non-medical to function effectively in achieving a timely diagnostic outcome, as well as seamless quality of patient care as the person as the patient journeys through the healthcare system. The ethics of each profession is important as collaboration and interdependencies increase (5) in an already complex evolving health system environment. DMI occupy an exceptional space and it serves an integral role in medicine. The rapid development and expansion of DMI have produced indisputable benefits to patients in terms of life expectancy and quality of life. Taking into consideration this inherent distributed diverse, and temporal nature of DMI services within a medical encounter and the ease of access, one cannot ignore the associated harm or risks with a referral for a diagnostic medical imaging examination (DMIE) and the outcomes thereof within the safety context. To practice medical imaging within a health system context at an exceptional level entails providing an effective and efficient culturally safe care and services.
The Distributed Nature of Medical Imaging Services
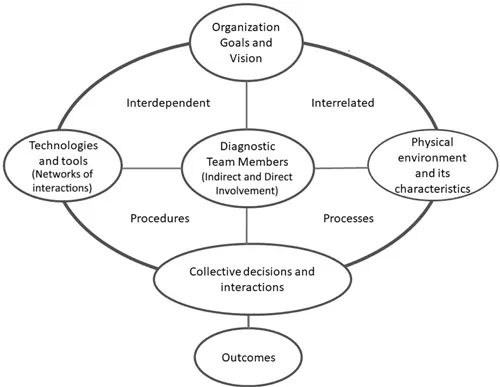
The best possible diagnostics, patient care, and care outcomes require multidisciplinary competences and thus interprofessional collaboration (4). Engineers, IT technicians, and physicists, among others, provide unique expertise to a DMI within a medical encounter (5). Enabling a seamless DMI service requires effective communication, meticulous cooperation, coordination, and collaboration through each point of contact with the patient and the HCP and between HCPs from the point of referral to the outcomes of their clinical diagnosis in mapping their treatment and management plans for the patients as persons within a health system context. Simultaneously, the process must be aligned with the organization’s goals, objectives, and values and professional regulatory body practice standards and professional code of conduct. So, each team member must have a collective understanding of the task at hand as their direct or indirect contribution is interdependent and interrelated with other team members as the patient journeys through and navigates various pathways of the healthcare system’s processes and procedures to achieve a quality health outcome (see Figure 1.1).
Figure 1.1 Illustrating the interconnectedness and interdependent nature of diagnostic medical imaging.
It is relatively easy for a radiographer, nurse, doctor, physiotherapist, or other professional to work in isolation and do their job without giving much thought to the bigger picture like the rest of the hospital and the service that patients receive. The case is similar for the engineers, medical physicists, and maintenance teams who need to ensure that the equipment is optimal in its functioning and the physical structure is safe and hazard-free depending on the financial resources. So, to provide this seamless high-quality care requires members of a multidisciplinary team to stay focused on their specific tasks and contribution to bridge a potential gap in care or else inadequate health services may result, affecting the realization of the ethical principles of beneficence (6).
Demonstrating clear cause-and-effect relationships between collaborative team behaviour and particular outcomes is often difficult (7). Ideally, the team should work together successfully with equality and balance, no team member should seek to dominate the team, team members should have trust and confidence in one another’s roles, responsibilities, and professional identity, and they should treat each other with respect, which Strudwick and Day call professional adulthood (5). Importantly, team members should recognize the different value perspectives, moral commitments, and priorities of the differing professions on the team, and they should feel safe to share and to defer professional autonomy to another professional. Furthermore, problem solving should be open and honest, flexible adaptable and team members should be able to work across professional boundaries (4). Of importance is being familiar with and understand the appropriate profession or discipline specific with its used language and terminology. If any of the aforementioned is compromised, interprofessional jealousy and conflicts could arise. In reality tribalism is unavoidable because every profession has its own occupational culture which differs from others, resulting in in-group and out-group behaviour and a tendency to classify the profession as “us” (e.g., medical practitioners) and all other groups as “them” (e.g., allied health professionals such as nurses and radiographers and radiologists). “They” are “the other”, and this “otherness” implies both differences and a different status. Most often the “other” (e.g., nurses and radiographers) is viewed as inferior or of less value than “us” (radiologists and medical practitioners) and is subject to stereotyping and prejudice (5).
As a typical example, the volume of radiology journal papers discussing, debating, and evaluating AI has increased exponentially since 2015 as radiologists quickly tackled initial concerns over role demise and extinction by writing counterarguments extolling the benefits of AI automation as an assistive and augmentative technology, not an existential threat. Radiographers are used to the fact that augmentation and support always focus on the radiologist rather than working together with the radiographers who are the mediators between the patient, referring medical practitioners (RMP), and the radiologist. One could argue that this upsurge in radiologist interest and debate was driven, in part, by role preservation and protectionism, but equally it has served as the voice that rationalized the value of the human worker within the imaging chain, a factor so easily overlooked in the quest for service and cost efficiencies (8). Frequently omitted both in clinical medicine and in radiology are the role and responsibilities of the radiographer often perceived as a mere button pusher.
This could be a lack of full awareness of the roles of other professionals, leading to prejudice and misunderstanding, and lastly mutual lack of education is often a cause of job tension. Newcomers to a profession construct a sense of their profession via legitimate peripheral participation and via discourse and learn their profession’s duties, boundaries, values, and aspirations. It is often during moments of tension, and the exchanges that follow, that judgements about “others” are formed. To overcome the issue of interprofessional conflict, Wiles et al. suggest that rather than focusing on the tensions of the multidisciplinary team the focus should be on dilemmas in a patient’s care. This means that rightness and wrongness are not necessarily determined by the actual outcome but by the quality of decisions and approaches used by the team in each situation because each team member involved might have different primary duties and concerns (6).
The Complex Medical Imaging Encounter and Associated Complexities
The DMIHCP’s role as a clinician is complicated, involving much more than simply performing DMIE, DMI intervention procedures, applying imaging protocols and evaluating and interpreting images; it also includes the communication of findings where applicable, quality assurance, quality improvement, education, policy-making, and many other tasks that cannot be performed by computer programmes. The wisdom and experience of these DMIHCPs is difficult to quantify and even more difficult to simulate with AI systems. The question is whether that accountability can be relinquished. The ability to deal with DMIE not only entails the nuanced use of clinical judgement, but also functioning in a constant flux faced with technological changes and advancements which directly influence the profession and clinical practice in terms of rapidly adapting and adopting advanced imaging opportunities to operate new technologies. Further the value proposition of DMIHCPs extends to before a diagnostic image is taken, important information about patient safety, radiation protection, pre-test probability, appropriateness, study protocol, and patient preparation need to considered in terms of medical physics, epidemiology, and health system context. A key role of the DMIHCP with the patient prior to the DMIE is to check and verify identification and indications for the requested DMIE to explain and inform the patient about the procedure of the examination to be undertaken. During the actual DMIE the interaction is focused on acquiring cooperation from th patient and coordinate the examination in acquiring an optimal quality image series. Post-DIME entails interaction on the outcomes of the examination a...
Table of contents
Cover
Half-Title
Title
Copyright
Dedication
Contents
Preface
About the Editor
Contributors
Chapter 1 Diagnostic Medical Imaging Services with Myriads of Ethical Dilemmas in a Contemporary Healthcare Context: Is Artificial Intelligence the Solution?
Chapter 2 Medical Imaging and Computer-Aided Diagnosis
Chapter 3 X- and Gamma Ray Imaging (CT, PET and SPEC, Scintigraphy, and Radiography): Benefits and Risks
Chapter 4 Cone-Beam Computed Tomography Applications in Dentistry
Chapter 5 Role of Nanoparticles in Medical Imaging
Chapter 6 Nanobiosensors and Their Applications in Medical Diagnosis and Imaging
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Medical Imaging Methods by Ashutosh Kumar Shukla in PDF and/or ePUB format, as well as other popular books in Medicine & Biotechnology in Medicine. We have over 1.5 million books available in our catalogue for you to explore.