FIRST PRIZE Winner in the Oncology category of the 2010 BMA Medical Book Competition. Intensive research over the last fifteen years has yielded a vast expansion in our understanding of the role of inheritance and genetics in a variety of cancers. Several inherited conditions have been identified which result in a high risk of various cancers; some of these were previously recognized, but the genetic basis underlying them has now been elucidated. This knowledge is now entering the sphere of routine clinical care. Surgeons, gastroenterologists, gynaecologists, oncologists, endocrinologists and many others need an awareness of these disorders, an understanding of genetic testing and when it is indicated, and how to manage patients with inherited cancer predisposition and their families. This book covers the basic concepts of cancer genetics. The common inherited cancer syndromes are each dealt with in greater depth, with the current management outlined. This book is aimed at all clinicians who may encounter these conditions in their practice. It aims to facilitate identification of high-risk individuals and families, to inform interaction with geneticists and other subspecialists, to provide a basis for patient management and to stimulate interest in these fascinating conditions.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineChapter 1
Genetics is not complicated
Background
There is something wonderfully simple about writing instructions in a universal alphabet of only four letters that provide descriptive words, all three letters long, for the amino acids which make up the proteins of the body or for the punctuation marks (Table 1). The challenge for the clinician is connecting the basic anatomy of genes through to the patient who just told you that they are the third person in the family to have a particular illness, or worse still that they are worried about their risk of a syndrome you have never heard of. Added to this longstanding cause of anxiety is the realisation that there may now be a genetic test for this condition but you are not sure how to organise it.
| Table 1. Genetic code - some examples. | |
| Amino acid | DNA base coding sequence |
| Alanine | GCT, GTT, GTA, GCG |
| Methionine | ATG |
| Isoleucine | ATT, ATC, ATA |
| Lysine | AAA, AAG |
| Stop codon | TAG, TGA, TAA |
Clinicians approach problems on a ‘need to know’ basis and remember information best when it relates to a clinical problem. These introductory pages are a reminder of the basic language needed to make sense of the later sections and are not intended to be comprehensive. A reading list of good genetics textbooks and useful reference sources is provided at the end of the chapter.
Genetic disorders are not rare
There is no doubt that there are many vanishingly rare disorders with a genetic basis, upwards of 6,000 of them. My favourite at the moment is a dominant trait called Birt Hogg Dube syndrome which carries a risk of renal cancer. The fact that there are so many rare disorders contributes to the assertion that this is not a rare problem. A survey in a Canadian population added together all the people who presented with a single gene defect or a major malformation and discovered that one in 20 people will have developed or died from a genetic disorder by the age of 25 years. Add to this the later onset conditions like hereditary breast and colon cancer and the fact that a major disease in a younger person will have a big impact on their whole family and associated clinicians, and it is obvious that, collectively, genetic disorders are very common, especially in developed countries where infectious diseases and malnutrition present fewer problems.
Chromosomes
Long before the recognition of the importance of DNA, early microscopists recognised that the thread-like ‘coloured bodies’ or chromosomes visible in the nuclei of dividing cells (Figure 1) clearly had something to do with transmission of hereditary information. Surprisingly, it was not until 1956 that it was established that human cells contain 46 chromosomes, by which time the anatomy had become clearer.

Figure 1. Normal male human karyotype.
Structure
Each of the 23 pairs of chromosomes is a long DNA molecule, coiled around histone proteins, then coiled and coiled again (Figure 2). When we see the familiar karyotype (Figure 1) in textbooks we are looking at a brief moment when the chromosomes have become supercoiled and are in a duplicated state. The cells are poisoned with colchicine to hold them at this point, when they are most easily examined and identified, based on the characteristic banding pattern produced by the physical and chemical interaction of the chromosomes with Giemsa stain.
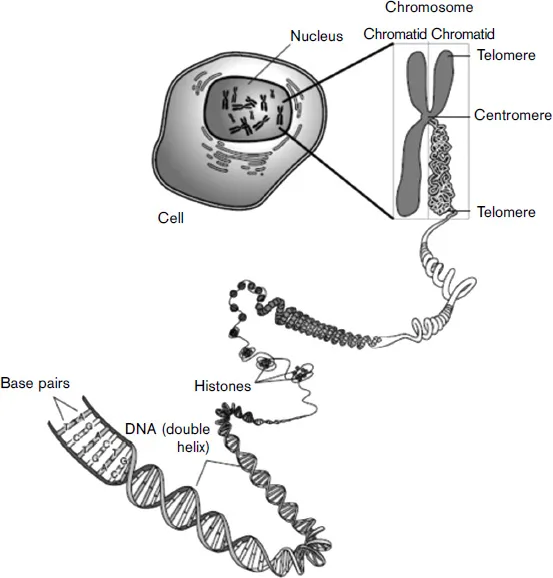
Figure 2. Chromosome structure. Reproduced under the GNU Free
Documentation License (GFDL).
(http://creationwiki.org/GNU_Free_Documentation_License).
Documentation License (GFDL).
(http://creationwiki.org/GNU_Free_Documentation_License).
It is this banding which gives rise to the positional nomenclature of genes within chromosomes. For example the APC gene is positioned at 5q21. This means that it is on chromosome 5, on the long arm of the chromosome (q denotes locations on the long arm of a chromosome, and p locations on the short arm). 21 denotes band 1 in region 2, these locations being defined by the visible banding of the chromosome. This is shown in Figure 3.

Figure 3. Ideogram of chromosome 5.
In years to come, the ‘old fashioned’ photograph of matching pairs of chromosomes will give way to a synthetic picture constructed by breaking up a person’s DNA and hybridising it to short fragments of the genome arranged on a slide. By competing the patient’s DNA with a population sample it becomes possible to identify missing bits and extra bits. This technique is rapidly falling in price and is extremely sensitive - in some cases too sensitive. It turns out that humans have chunks of DNA which can be repeated multiple times without clinical effect, so in future there will be much debate about ‘chromosomal variants of uncertain significance’.
Conversely, tiny deletions and duplications which are significant will potentially lead us to genes of clinical importance in certain clinical situations. The most dramatic example in colorectal surgical history was the case report of a man with a chromosome 5 deletion and learning disability who also suffered from familial adenomatous polyposis (FAP), an observation which led to the identification of the location of the causative gene and shortly thereafter the APC gene itself.
Genes
Often a gene and the protein that it codes for will have the same name. In order to differentiate them italics are used when referring to the gene, and not when referring to the resulting protein (e.g. the APC gene codes for the APC protein).
We use the word ‘gene’ in two interchangeable ways. It can refer to a section of one of the 23 pairs of chromosomes or it can refer to a faulty segment of DNA which results in a disease. Thus, we speak of the K-ras gene, or more precisely the K-ras gene locus and we speak about the ‘gene’ responsible for FAP, which refers to a defective copy or allele of the APC gene on chromosome 5. When we use the terms dominant and recessive we are discussing alleles at a particular locus.
Dominant or recessive?
When Mendel solved the puzzle of inheritance with his pea plants, he coined the terms dominant and recessive to describe the two basic types of genes, or ‘factors’ as he called them. As the name suggests, a dominant gene manifests itself in the presence of a recessive gene. The effect of recessive genes, on the other hand, are only seen when there are two copies present.
The situation is further confused by the use of the term dominant to refer to a clinical phenotype or syndrome. Until his death in 2008, Victor McKusick spent over 40 years compiling his textbook, Mendelian Inheritance in Man, which has become a free online resource (www.ncbi.nlm.nih.gov/sites/entrez?db=omim). The many thousands of dominant and recessive phenotypes are catalogued along with links to causative genes where known. Many of these phenotypes earn their title on the basis of inheritance pattern. Classically, a dominant trait will be transmitted to half, on average, of the offspring of an affected individual. If a characteristic pattern runs through three generations, this is taken as strong evidence of a dominant gene defect. Recessive gene defects are characterised by occurring in one generation, affecting on average one in four of siblings. This is because each parent is a carrier and each has a half chance of passing on the defective gene so a child has half of a half, or a quarter chance, of receiving two defective copies and developing the disease.
In the field of colon cancer FAP is a classic dominant and mutY human homologue (MYH)-associated polyposis or MAP is a classic recessive. It is of historical interest that the term ‘familial’ used to be synonymous with what we now call recessive traits while ‘hereditary’ refers to dominant traits. The surgeons responsible for coining the term FAP were clearly unaware of this usage; it should have been HAP!
When family trees are examined in close-up many exceptions emerge. The most obvious in these days of reduced family size and rare cousin marriage is that most examples of recessive and dominant inheritance will be isolated cases. Many dominant traits which are not compatible with reproduction are never seen in two generations.
New mutations
Some, or in some conditions all, cases occur as new mutation...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Foreword
- Chapter 1: Genetics is not complicated
- Chapter 2: Genetics and cancer
- Chapter 3: Ethical and legal aspects of cancer genetics
- Chapter 4: Familial adenomatous polyposis
- Chapter 5: MYH-associated polyposis
- Chapter 6: Lynch syndrome (hereditary non-polyposis colorectal cancer)
- Chapter 7: Breast cancer
- Chapter 8: The gynaecologist and inherited cancer
- Chapter 9: Multiple endocrine neoplasia syndromes
- Chapter 10: Neurofibromatosis
- Chapter 11: Familial gastric cancer
- Chapter 12: Familial pancreatic cancer
- Chapter 13: Hamartomatous polyposis syndromes
- Chapter 14: The future structure of care: cancer genetics
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access A Guide to Cancer Genetics in Clinical Practice by Clark, Sue in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.