This book is a topical review of venous disease providing an up-to-date view of management and current issues. It is aimed at professionals involved in the management of patients with venous disease, whether they be a vascular specialist, nurse or technologist, physicians with an interest in venous disease, as well as primary care doctors and nurses who wish to complement their knowledge of the area. Acknowledged experts, active in the field, have covered topics ranging from the history, epidemiology, signs and symptoms, investigation and treatment of venous disease to issues of quality of life, complications and litigation, and setting up a clinical service. The treatment of deep vein thrombosis is discussed together with the controversial area of DVT and travel. Newer techniques of vein ablation, subfascial endoscopic perforator surgery (SEPS) and foam sclerotherapy are also covered. This book should find a place on the bookshelf as an exciting review of contemporary themes and complements traditional textbooks.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaChapter 1
The history and importance of
venous disease in modern practice
Introduction
The modern management of venous disease is inextricably linked with advances in physiological measurement and imaging. Indeed, early accounts of disorders describe anomalies and only in the mid-20th century was there an attempt to merge ‘form and function’. Varicose veins have been reported for thousands of years with one of the earliest accounts of serpent-shaped dilatation of the lower limbs from about 1552BC in the Ebers papyrus (Figure 1). The first reliable description of intervention for extremity varices appears in a Turkish textbook, Imperial Surgery, written in 1465AD, although procedures appear to have taken place during the earlier Byzantine period. A published case history of venous thrombosis is recognised at the Bibliothèque Nationale in Paris, affecting a Normandy man aged 20 years in 1282AD. The patient sustained unilateral oedema with ulceration and exudation, and although able to walk only with crutches initially, the symptoms eventually settled leaving only mild long-term leg throbbing. Probably the most significant early work was by Fabricus in 1603 and his student Harvey in 1628, who described the structure and function of venous valves and the circulatory system respectively (Figure 2).

Figure 1 The Ebers papyrus was discovered in Egypt in the 1870s and contains 877 recipes for diseases or symptoms.
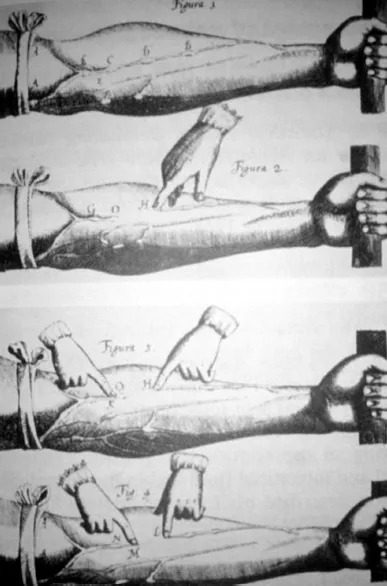
Figure 2 Illustration of venous valves from Harvey’s 1628 book De Moto Cordis.
Paré in the 16th century underpinned surgical principles and these were developed by Trendelenburg (Figure 3) and others around the beginning of the 20th century, leading to Keller and Mayo in 1905/6 performing the first ablation of the great saphenous vein, thus providing a gateway to the modern era 1, 2.
Figure 3 Friedrick Trendelenburg (1844-1924) was Surgeon-in-Chief at Leipzig.
Courtesy of www.historiadelamedicina.org.
Courtesy of www.historiadelamedicina.org.
Historical landmarks
Investigation of venous disorders
Clinical examination with use of the Trendelenberg test and tourniquet has been the mainstay of diagnosis of superficial venous incompetence, even in recent years, despite the inaccuracies in differentiation of saphenopopliteal and perforator disease. The recognition of the physiological implications of deep venous incompetence remained elusive until the era of pulsed Doppler ultrasound imaging and flow measurements. Plethysmography was developed in the mid-20th century and is based upon measurment of venous refill times using strain gauge, electrical impedance or skin colour changes. Difficulties with reproducibility and standardisation has meant that plethysmography has limited use in clinical practice but is valuable in venous research, particularly where continual assessment of individual patients is required.

Figure 4 Ascending venogram with thrombus in the femoral vein.
Contrast venography was popularised in the 1960s and even now is regarded by many as the gold standard for the diagnosis of deep vein thrombosis (Figure 4). Descending femoral venography enabled diagnosis of deep venous incompetence based upon distal reflux of contrast, although the clinical implications of single or multiple valvular reflux are not clear. Venography or phlebography is still of value in planning surgery for pelvic venous obstruction and determining the origin of atypical lower limb varicosities, but its use has largely been superseded by duplex imaging.
Continuous-wave Doppler ultrasound has been used in fluid engineering since the 1950s and was further developed, initially in arterial disease where the velocity shifts are significant, by Satomura in the 1970s, when the importance of ankle/brachial systolic pressure indices was recognised. Strandness popularised the technique in both arterial and venous disease, but now modern duplex ultrasound systems combine flow measurement with imaging, enabling the function of individual valves to be identified whilst examining the quality of vein wall, as well as identifying deep vein thrombosis 3. The accurate assessment of perforator and pelvic vein incompetence has led to dilemmas in the significance, and need for treatment, of these conditions. Initial early concerns over the size of ultrasound equipment have been addressed by development of portable devices, although considerable operator training and experience is required. Hand-held Dopper devices, measuring flow alone, are useful as an adjunct to clinical examination but have limited specificity in determining saphenopopliteal and deep vein incompetence. Both duplex imaging and Doppler flow assessment have ensured that surgery for venous incompetence can be planned and is appropriate with venous surgeons recommending that all patients undergo pre-operative investigation.
Modern imaging techniques such as CT angiography have found a place in the diagnosis of pulmonary emboli, whilst magnetic resonance venography may be useful in the management of pelvic and thoracic outlet venous obstruction in the future.
Sclerotherapy and other local treatments
Sclerotherapy was commenced by Pravaz in approximately 1860 and promoted in Europe in 1947 with the foundation of Sociètè Francaise de Phlebologie. Fegan subsequently popularised and developed the technique that bears his name, although by the late 20th century enthusiasm, certainly in the UK, was reducing 4. The reasons for this were the recognition that sclerotherapy did not address the underlying valvular incompetence, leading to high recurrence rates reported as 90% at ten years, patient acceptability of prolonged compression and complications of the technique including ulceration and skin staining. Recently, the development of less toxic intravenous agents and the introduction of foam sclerotherapy under duplex guidance has led to a renaissance of the procedure. Foaming of the sclerosant enables the injection to remain within the targeted vein and can be accurately followed to the saphenofemoral junction. Trials of the technique are underway but if long-term recurrence rates are low then traditional surgery will be challenged. Within Europe the practice of phlebology is widespread leading to a new specialty for venous disease that is not found in the UK.
The rise in demand for cosmetic surgery has led to increasing requests for treatment of telangiectasia or ‘spider veins’. These are mainly present on the legs and can be unsightly, but normally are asymptomatic. A number of techniques are available including fine needle sclerotherapy using loupes and a 30-gauge needle, photodynamic therapy and laser. The result is not predictable on an individual basis and recurrence is usual as this is a progressive disease.
Surgery for varicose veins
Trendelenberg in 1891, described ligation of the great saphenous vein in the mid-thigh as a treatment for varicose veins, but the significance of flush saphenofemoral ligation was not appreciated until 1904 when Tavel indicated the advisability of this procedure in order to prevent recurrence. It was not until 1906 that Keller and Mayo described stripping with the operative techniques refined by Turner Warwick in the 1930s. Linton at same time published an account of the classic subfascial ligation of the perforating veins with a revival by Cockett in 1953 who applied a similar technique to the treatment of venous ulcers 5. The problems of operating through the infected ulcer base to ligate the perforators has been overcome with the recent development of Subfascial Endoscopic Perforator Ligation (SEPS) but even so, the procedure remains controversial with much debate over the significance of incompetence at this site (Figure 5).
Contrast imaging initially confirmed the importance of flush ligation of incompetent valves in order to prevent recurrence, but duplex ultrasound now ensures that visualisation is both sensitive and non-invasive. Latterly, not only is the need to treat Hunterian thigh perforators and the Giacomini vein recognised, but vulval varicosities, pelvic tributaries and other minor branch incompetencies have been identified, posing dilemmas as to the need for ligation which are still debated today. The 1980s were concerned with the prevention of recurrence after saphenofemoral ligation. Initially all recurrence was attributed to incorrect surgery and inability to ligate all branches of the saphenofemoral junction, particularly when the majority of varicose vein surgery at that time was performed by t...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Contributors
- Preface
- Chapter 1: The history and importance of venous disease in modern practice
- Chapter 2: Epidemiology of venous disease
- Chapter 3: Signs and symptoms of venous disease
- Chapter 4: Investigation of venous disease
- Chapter 5: Quality of life and outcome assessment in patients with varicose veins
- Chapter 6: Quality of life in patients with venous ulcers
- Chapter 7: Primary varicose veins: minimising complications, complaint and litigation
- Chapter 8: The management of recurrent varicose veins
- Chapter 9: New methods of vein ablation
- Chapter 10: Subfascial endoscopic perforator surgery (SEPS)
- Chapter 11: Sclerotherapy for venules and their feeder veins
- Chapter 12: The prophylaxis and treatment of venous thrombo-embolism
- Chapter 13: Venous reconstruction: indications and success rates
- Chapter 14: The role of nurse-led clinics
- Chapter 15: Venous leg ulcer services: organisation, diagnosis and role of surgery
- Chapter 16: Deep vein thrombosis and travel
- Chapter 17: Foam sclerotherapy
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Venous Disease Simplified by Davies, Alun, H,Lane, Ian,Lees, Tim, Davies, Alun, H, Lane, Ian, Lees, Tim in PDF and/or ePUB format, as well as other popular books in Medicina & Teoría, práctica y referencia médicas. We have over 1.5 million books available in our catalogue for you to explore.