This book will help you take a badly wounded patient to the operating room, organize yourself and your team, do battle with some vicious injuries and come out with the best possible result. It is a practical guide to operative trauma surgery for residents and registrars, for general surgeons with an interest in trauma, and for isolated surgeons operating on wounded patients in military, rural or humanitarian settings. A surgical atlas may show you what to do with your hands but not how to think, plan and improvise. Here you will find practical advice on how to use your head as well as your hands when operating on a massively bleeding trauma patient. The first part of this book presents some general principles of trauma surgery. The second part is about trauma surgery as a contact sport. Here we show you how to deal with specific injuries to the abdomen, chest, neck and peripheral vessels. The single most important lesson we hope you will derive from this book is to always keep it simple because, in trauma surgery, the simple stuff works.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 4
The Crash Laparotomy
Damn the torpedoes, full speed ahead!
~ Admiral David J. Farragut
In most surgical training programs, you spend much time in the OR with the cautery in hand, merrily blasting away at stray erythrocytes while your teacher unobtrusively opens the correct tissue planes with a right-angled clamp, an ever-present sucker tip or an educated finger, pretending you are doing the case. The way you cut tissue, tie knots, arrange retraction, and suture bowel are all part of the technical language of general surgery.
A trauma operation is not an accelerated version of the elective procedure. It requires a different technical language and, most importantly, a different mindset. In this chapter, we demonstrate these differences by taking a familiar operation, exploratory laparotomy, and translating it into the technical language of trauma surgery. Rapid alternations between swift, crude exposure maneuvers and meticulous dissection are the hallmarks of a trauma laparotomy. It's like dancing through a real minefield while playing DOOM™ on your laptop. Get the picture?
The operative sequence
Every trauma laparotomy follows the same methodical, practiced operative sequence.
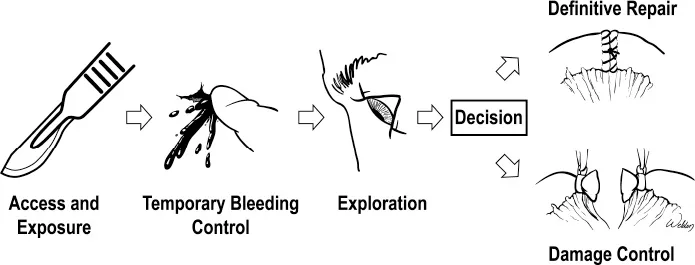
The key decision in this algorithm is the choice between definitive repair and damage control. The earlier you make this decision, the better for the patient.
Gaining access
Enter the peritoneal cavity through a long midline incision, the Texas name for which is "Hey diddle diddle, right down the middle.” The less stable the patient, the faster you should dive in. Take the scalpel and make a bold cut through the skin and subcutaneous tissue. If you grab the diathermy to systematically barbeque subcutaneous bleeders in a patient with a systolic pressure of 60, you are probably in the wrong specialty and should consider a career change. The hypotensive trauma patient is peripherally vasoconstricted, and you are wasting time on nonsense oozing while rapid intra-abdominal bleeding continues unabated 2cm below the tip of your diathermy. Sounds pretty stupid because it is.
The incision begins below the xiphoid, skirts around the umbilicus, and ends above the pubis. An experienced surgeon uses three long and precise passes of the knife to enter the peritoneal cavity. The first sweep gets you past the skin and into the subcutaneous tissue. The second pass lands you on the linea alba. Develop the ability to gauge the depth of the subcutaneous fat and the "feel" of landing on the fascia without cutting it. The third and last pass of the knife divides the linea alba to visualize the preperitoneal fat.

Train yourself to make the incision like a pro. If it takes you five or six sweeps, you are okay but not yet ready for prime time.
The key maneuver is to cut in the midline where the abdominal wall is thinnest and entry into the abdomen is quickest. This is called “gaining the midline.” A good marker of the midline is the decussation of the fibers of the anterior rectus sheath. If you see muscle underneath your fascial incision, steer medially.
Now, take advantage of a little-known anatomical fact. In most patients, the peritoneum just cranial to the umbilicus is either very thin or has a defect. There is only very thin preperitoneal fat in this area, making it the ideal spot for entering the peritoneal cavity. Forget the elaborate dance (often taught in elective surgery) of picking up the peritoneum between two pairs of pickups and making a small nick to let air in. Simply poke a finger into this peritoneal defect immediately above the umbilicus, and you find yourself in the peritoneal cavity.

Using a pair of heavy scissors, cut the peritoneum, together with the overlying preperitoneal fat, to the full extent of the incision. Use your non-dominant hand to push the intestines down to protect them from your advancing scissors. Identify the falciform ligament and divide it between clamps to gain access to the right upper quadrant. You're in the belly, ready to Rock n' Roll.
Enter the belly with three sweeps of the knife and one educated finger
A word of caution
The major pitfall during a crash laparotomy is iatrogenic injury. The left lateral lobe of the liver, the small bowel, and the bladder are in jeopardy in the upper, middle, and lower parts of the incision, respectively. On a particularly bad day or if you are especially gifted, you can injure all three organs in one bold sweep.
If the patient has a pelvic fracture, entering a pelvic hematoma is generally considered a bad move. Make an upper midline incision, carefully peek into the abdomen, and extend your incision downward below the umbilicus under direct vision.
Entering the abdomen through a previous laparotomy scar can be time-consuming and exasperating in a hypotensive patient. The safe technique is to extend the incision beyond the old scar into virgin territory and enter the peritoneal cavity where adhesions are less likely. Then, open the old scar piecemeal, after making sure that the undersurface is clear and pushing adherent loops of bowel out of the way. Even if you have completed your incision without mishap, you may still face adhesions of bowel loops to the anterior abdominal wall. When these adhesions are dense or multiple, you will feel a little stupid engaging in careful adhesiolysis while the anesthesiologist is pumping unit after unit of blood into your hypotensive patient. Is there a quicker way in? Yes, there is.
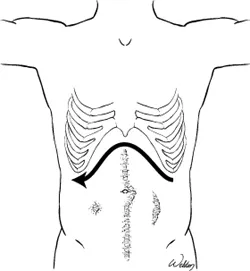
A creative solution in an abdomen with multiple old scars would be not to enter in the midline, but make a bilateral subcostal incision (also known as a Double Kocher or a rooftop incision). The incision itself takes longer to make and close, but you will more than make up for it by skirting around the troublesome midline adhesions.
Stay away from old scars
Once inside the abdomen
When you first peek into the open abdomen, all you can see is a spaghetti of bowel loops swimming in a pool of blood and clots. Your first priorities are to achieve temporary hemostasis and evacuate the blood so you can see what is going on.
The key maneuver now is evisceration. Rapidly gather the small bowel loops outside the abdomen toward you (to the right and up). Don't just shove laparotomy pads into the open abdomen without eviscerating the bowel, an act akin to throwing paper napkins into a bowel of soup - and a total waste of time. Evisceration converts the bloody mess into a manageable work space, allowing you to see what you are doing. Rapidly evacuate the blood and achieve temporary hemostasis.

Eviscerate the bowel early
Choose a temporary hemostatic technique based on the mechanism of injury. In blunt trauma, begin with empirical packing. Hand your assistant a large retractor to elevate the abdominal wall of each quadrant in turn, and pack the abdomen rapidly. Begin with the right upper quadrant by placing your left hand over the dome of the liver, pulling it gently toward you, and placing packs over your hand above and then below the liver. Pack the right paracolic gutter. Move to the left and put your non-dominant hand above the spleen, pulling it gently toward you, then pack over your retracting hand above the spleen and left lobe of the liver. Create a sandwich by packing medial to the spleen. Move to the left paracolic gutter and then to the pelvis, and pack them. All this time, the eviscerated bowel remains out of the way. If blood is accumulating on the eviscerated bowel, the source is a mesenteric bleeder. Deal with it directly. During packing and while your non-dominant hand is retracting and protecting the liver and spleen, feel for any obvious injury, and begin planning your approach b...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Introduction: What this Book is all About
- Section I: - Tools of the Trade
- Section II: - The Abdomen
- Section III: - The Chest
- Section IV: - The Neck and Extremities
- Epilogue: The Joy of Trauma Surgery
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access TOP KNIFE: The Art & Craft of Trauma Surgery by Hirshberg, Asher,Mattox, Kenneth, L in PDF and/or ePUB format, as well as other popular books in Médecine & Théorie, pratique et référence de la médecine. We have over 1.5 million books available in our catalogue for you to explore.