Vitreoretinal (VR) surgery has steadily evolved over the years and this handbook provides a comprehensive overview about its past, present and future. It covers a wide array of topics ranging from its fascinating origins to recent technological advances, from surface anatomy to their clinical relevance, from anaesthesia to building and maintenance of operation theatre, from major surgical steps to sub-steps, from preventing to managing complications, and from routine surgeries to rare surgeries. Included in addition is a section on futuristic surgeries and another on important studies in relation to vitreoretinal surgery. Hence, Handbook of Vitreoretinal Surgery serves as a ready reference for both fledgling and experienced VR surgeons in this exciting field of ophthalmic surgery.
.
Key Features
Includes recent developments like 3D surgery, telescopic IOL, bionic implants and robotic surgery.
Highlights the importance of surface anatomy and provides a deeper view into the working of vitreous machines, microscopes and other surgical components.
Text is supported with videos of rare surgeries like endoillumination-assisted scleral buckling surgery, placement of retisert intravitreal implant, suprachoroidal drug injection, intralesional injection into a subretinal abscess and endoillumination-assisted biopsy of intraocular mass lesions.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
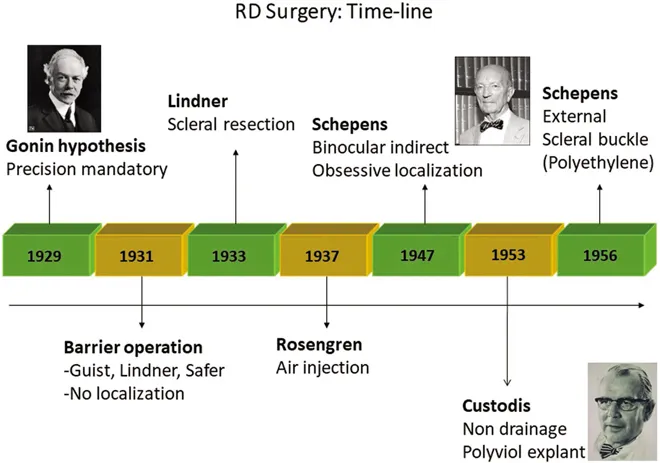
The first step towards tackling retinal problems through surgery, in a logical and systematic manner, was taken by Jules Gonin [Figure 1.1]. He was the first to propound that retinal detachment was caused by a tear in the neurosensory retina and that surgical closure of these would result in successful reattachment of the retina. His approach of search a break, seek a break, and seal a break [3S] still remains the cornerstone of retinal detachment surgery. It is ironic that it took more than a decade for his views to become widely accepted. It soon became established that retinal detachment could be successfully repaired by accurate localization of the retinal tear, external drainage of accumulated subretinal fluid, induction of sterile inflammation around the region of the tear, and then supporting the tear externally by an encircling element. Some of the methods used to achieve sterile inflammation were ignipuncture and chemical cautery. The first description of using an external support was made by Jess [1937] in Germany [a gauze pad was used as a temporary indent]. Scleral buckling using an episcleral implant was first conducted by Custodis [1949]. He was also instrumental in introducing Polyviol as an explant material [1953] and later for the concept of non-drainage retinal detachment surgery.
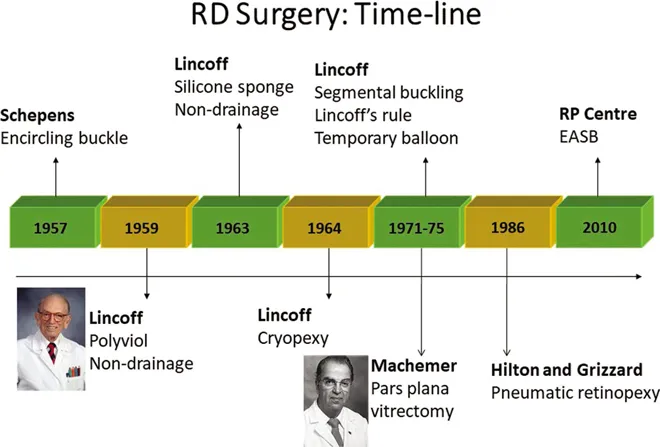
However, a major limitation for the concept to gain traction was the inability to visualize the peripheral retina and locate the retinal tear(s), owing to the narrow field of view provided by available ophthalmoscopes. The problem of difficulty in visualization of the retinal periphery, wherein most retinal breaks are located, was solved with the pioneering work of Charles Schepens, who introduced the binocular indirect ophthalmoscope [1947] and propagated the application of contact fundus biomicroscopy. In addition, it was realized that materials such as Polyviol, used for indenting the sclera, were not optimal and were themselves causing tissue damage. So, Schepens initially used polyethylene tubing [1957] as a material for providing external support. Initially, the support was only to the region of the tear and for a clock hour on either side. The barricade with polyethylene was called a scleral buckle. But failures were observed because of leak across anterior part of the tear. To overcome this anterior leak, the buckle was extended to 180 degrees and thereafter to 360 degrees, thereby introducing the concept of encirclage [1957]. When this failed to reduce the leakage, it was decided to increase the width of the scleral buckle. However, the concept of encirclage has remained because it may retain the height and position of the buckle and counter tractional forces from the anterior vitreous. To anchor the external plombage, partial-thickness tunnels were made in the sclera. A year later, Arruga [1958] reported using Supramid, Mersilene, and nylon sutures instead of polyethylene tubing. Silicone was first used by Girard [1959] for scleral indentation [as a rod made of silicone rubber]. It was again Schepens and his team who first reported the use of solid silicone as buckling material [1960]. They developed several designs of buckle, some of which are still being used. Lincoff Harvey [1965] and his team used silicone sponge to treat large breaks, and these were in use until the late 1990s. With advances in vitreoretinal surgery, large tears and radial tears are now better managed with an internal approach, so silicone sponges have lost their importance. Major disadvantages of silicone sponge were the high risk of infection because of the air pockets and extrusion. Hydrogel buckle [1972] and expandable silicone [1973] were described by Grignolo and Banuelos, respectively. Two types of balloon implants have been used in the past: permanent and temporary. The first permanent [sutured] balloon implant to support the macula was reported by Hoepping as early as 1969. Currently, macular buckling seems to be regaining attention for management of macular pathologies in patients with high myopia. Use of a temporary [sutureless] balloon buckle was tried by Lincoff in 1979.
Methods to induce sterile inflammation around the retinal tear have included thermal cautery [ignipuncture, Gonin, 1930], chemical cautery using potassium hydroxide sticks [Guist, 1931; Lindner, 1931], electro-diathermy [Safar, 1931], and diathermy electrode. Multiple diathermy burns were applied to the bed of a partial-thickness scleral flap created over the location of the tear. After a series of explant related infections, Lincoff undertook some experimental studies, which revealed that the cause of infections was not directly related to the silicone sponge but to diathermy. He established that diathermy had a tissue-destroying effect and often caused scleral necrosis with its associated complications. Subsequently, curious about the carbon dioxide probe being used by his dermatologist, Lincoff introduced cryotherapy [see section on cryotherapy] as a method for inducing sterile inflammation during retinal detachment surgery. However, CO2 was not conducive for use within the orbital spaces. So, Lincoff and Mclean modified a nitrous oxide cryoprobe being used by neurosurgeons and applied it to retinal detachment procedures [1964]. Very soon cryopexy replaced diathermy and became the method of choice to induce retinopexy. Unlike diathermy, cryotherapy had no damaging effect on the scleral fibres and could also be safely applied across an extraocular muscle, with no lasting complication. Lincoff also introduced silicone buckle as a better alternative to Polyviol. These landmark contributions significantly reduced the complications of retinal detachment surgery. Lincoff was also instrumental in throwing light on the pioneering work of Custodis, in successfully treating retinal detachment without external drainage of subretinal fluid [non-drainage surgery]. Having spent time with Custodis in his clinic and noticing the successful outcomes, Lincoff introduced non-drainage surgery into his own practice in New York. Until then, external drainage of subretinal fluid through a scleral cutdown was routinely practiced despite some serious adverse effects that could result. In the course of analyzing the first 1000 cases of retinal detachment treated using silicone buckle and cryopexy, Lincoff and Gieser provided guidelines for preoperative localization of the retinal break based on configuration of the retinal detachment [Lincoff’s rule, 1971].
Figure1.1 Timeline in the evolution of retinal detachment surgery.
Despite high success rates [90%] with this procedure, failures were noted at a higher rate in patients with large tears. It was observed by Norton [1973] that the reason for this was leakage through radial folds that developed along the posterior margin of large tears following surgery with a segmental buckle. To counter the radial folds, he suggested injection of air into the vitreous cavity, thus reviving an approach that was first reported by Rosengren [1938] several decades earlier. The short half-life of air within the vitreous cavity was a limitation, so efforts were made to seek inert and biologically compatible gases with longer duration of action. The half-life of a gas within the eye was identified to be related to their solubility. This led to evaluation with short-chain perfluorocarbon gases on the suggestion of a chemical engineer, Andrew Lincoff [1984]. In the next few years, after the introduction of perfluorocarbon gases to salvage some failures following scleral buckle, Hilton and Grizzard [1986] described a new approach for primary management of simple retinal detachments. This technique, termed pneumatic retinopexy by the authors, continues to polarize retina surgeons about its utility, even to this day. The concept of using iso-expansile mixture of perfluorocarbon gases as vitreous substitutes at the end of surgery was introduced by Gary Abrams. Evaluation with long-chain perfluorocarbons [which are liquids] began soon after the work on perfluorocarbon gases. Heavy liquids were, however, approved only later for use as an intraoperative adjunct to achieve temporary tamponade following evaluation of its utility by Chang Stanley, Lincoff, and colleagues [1989]. Haidt had, however, used perfluorocarbon liquid with vitreous surgery much earlier in 1982.
While these approaches to managing retinal detachment from an external route were in progress, some other pioneers were working on solving severe visual problems resulting from conditions such as non-resolving vitreous haemorrhage. Until about half a century ago, it was firmly believed that the vitreous contributes to the structural integrity of the eye, and its removal would result in permanent damage. Owing to serendipity, however, David Kasner [1969], while conducting experimental work on cadaver eyes in his garage, noted that vitreous could be removed using forceps and scissors. He soon applied this technique to the removal of vitreous that prolapsed out of the posterior chamber during intracapsular cataract surgery [calling it radical anterior vitrectomy]. He then realized that vitreous removal may also be helpful in patients with significant opacities in the vitreous, so he went on to undertake this procedure in two patients, one with vitreous amyloidosis and the other with vitreous haemorrhage. This approach, which he called open sky vitrectomy, involved making a 300-degree limbal section and flipping over the cornea before dissecting the vitreous. Significant improvement was noted in patients following open sky vitrectomy. David Kasner taught cataract surgery to residents at the Bascom Palmer Eye Institute and lectured about his research findings, including the outcomes on patients with vitreous opacification. During one such meeting, Robert Machemer [1971], a faculty member at the same institute, was intrigued by the ability of the eye to tolerate significant removal of the vitreous without resulting in serious damage. Following a few visits to Kasner’s garage to observe his research work on vitreous removal, Machemer conceptualized the idea of removing the vitreous through a closed approach using a rotatory, motorized cutter. Then, Machemer along with his colleague, Buettner, and an instrument design expert, Parel, developed multiple prototypes of a motorized vitreous cutter. Initial experiments were conducted on eggs and involved removing the white without damaging the yolk or shell, using the innovative device introduced through a hole in the shell. The final version of this came to be known as VISC [vitreous infusion suction cutter] because it performed multiple functions of infusing fluid into the vitreous cavity, cutting of the vitreous fibrils and aspirating the fragments out of the eye [Figure 1.2]. This probe had an external diameter of 2.3 mm and a single 17G port [1.5 mm] and hence needed a large scleral incision [Video 1.1]. Infusion of fluid was driven by gravity, and suction was provided by manual aspiration through a syringe; only the cutting was motorized. The initial vitrector was prone to cause winding of the vitreous fibrils and was soon replaced by an oscillatory vitrector [Roto Extractor]. Parel, a colleague of Machemer, was not only involved in the designing of VISC but also introduced fiberoptic endoillumination. Unknown to Machemer, Anton Banko is said to have patented a vitreous cutter prior to the VISC. In the very subsequent years, O’Malley and Heintz [1975] demonstrated the concept and superiority of vitrectomy using divided function 20G [0.9-mm] instrumentation, with separate pars plana opening for infusion, vitreous cutter [with aspiration], and endoillumination. They also introduced the first pneumatically driven vitreous cutter and active extrusion [by aspiration] through a foot pedal–controlled console system [Ocutome 800]. The first electric solenoid driven axial [guillotine] vitreous cutter was developed by Gholam Peyman. It is necessary to indicate here that both open sky vitrectomy and vitrectomy using a vitrector seem to have been reported a few years earlier in the Japanese literature. Ever since these developments, three port pars plana approach has become the accepted norm for vitreoretinal surgery.
Figure1.2 Timeline in the evolution of retinal detachment surgery. EASB, endoillumination-assisted scleral buckling.
A major shift in the drainage of subretinal fluid, from an external, transscleral route to an internal, transretinal route [by simultaneous air-fluid exchange] was introduced by Steve Charles, who went on to make several other immense contributions to vitreoretinal surgery, including endophotocoagulation, flute needle, power silicone injector, end-grasping forceps, diamond-coated membrane-peeling forceps, scissors segmentation, proportional or linear foot pedal control, xenon light source, servo-controlled intraocular pressure, proportional diathermy, the concept of system integration of all functions of the vitrectomy machine, no spring-dual actuation vitreous cutter, and so on. McEwen introduced the automated air pump to facilitate air-fluid exchange in a controlled manner [replacing the previous syringe-based method]. Retinectomy and submacular surgery were pioneered independently by both Machemer and Charles. For peeling of epiretinal membranes, Machemer used a bent pick, while O’Malley used a membrane pick [blunt margins], and Charles used end-grasping forceps. Yasuo Tano introduced the diamond-dusted membrane scraper. Chang, other than introducing perfluorocarbon liquid, also developed the dual-function, end-aspirating laser probe. Charles, along with Carl Yang, introduced the first 20G disposable, pneumatic guillotine cutter.
Further developments have revolved around adopting advancements in technology and material sciences to refine the functioning, precision, and control of vitreous machines as well as intravitreal instruments. Some of these developments include the introduction of first 25G [0.5 mm] by Eugene de Juan [1990] and colleagues, 23G surgery by Hilton [2002] and Klaus Eckhardt [2005], and 27G surgery by Oshima et al [2007]. The initial 25G system introduced by de Juan and Hickinbotham [first to describe a trocar cannula system] needed to be sutured. In 2002, Fujii and de Juan developed the first transconjunctival sutureless vitrectomy [TSV25] system. With the introduction of micro-incisional or small-gauge vitreous surgery, patient comfort and safety have significantly improved, and surgical time has substantially reduced, so much so that 20G vitreous surgeries have become rapidly relegated to the past. Improvements in the field of view of visualization lenses, including noncontact binocular indirect ophthalmic microscope by Manfred Spitznas and contact system [Advanced Visual Instruments] with stereo inverter by Stanley Chang, have also contributed to making vitreoretinal surgery safer by providing a panoramic view of the surgical field.
In addition to these advances, there has been a steady endeavor by vitreoretinal surgeons to extend the scope of retinal diseases in which surgery may be helpful. These conditions include conventional macular hole surgery by Kelly and Wendal [1991], macular hole surgery with internal limiting membrane [ILM] peeling by Yooh [1996] and Eckardt [1997], modified macular hole surgery [large, chronic] by Michalewska [2010], optic disc pit maculopathy by Bakri [2004], myopic foveoschisis by Benhamou [2002] and Kishi [2003], vitreomacular traction, resection of intra...
Table of contents
Cover
Half Title
Title
Copyright
Dedication
Contents
List of Videos and Legends
Foreword
Preface
Acknowledgements
About the Author
Introduction
Chapter 1 Milestones and Pioneers
Chapter 2 Training in Vitreoretinal Surgery
Chapter 3 Peri-operative Investigations
Chapter 4 Anaesthesia: Approaches and Limitations
Chapter 5 Operation Theatre: Design and Sterilization
Chapter 6 Surgical Anatomy and Other Considerations
Chapter 7 Machines and Instrumentation
Chapter 8 Adjuncts in Vitreoretinal Surgery
Chapter 9 Surgical Approaches and Steps
Chapter 10 Common Vitreoretinal Procedures
Chapter 11 Vitreoretinal Surgery in Rare Conditions
Chapter 12 Complications in Vitreoretinal Surgery
Chapter 13 Important Studies in Vitreoretinal Surgery
Chapter 14 Futuristic Approaches in Vitreoretinal Surgery
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Handbook of Vitreoretinal Surgery by Pradeep Venkatesh in PDF and/or ePUB format, as well as other popular books in Medicine & Emergency Medicine & Critical Care. We have over 1.5 million books available in our catalogue for you to explore.