
eBook - ePub
Stimulation of the Peripheral Nervous System
The Neuromodulation Frontier
- 244 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Stimulation of the Peripheral Nervous System
The Neuromodulation Frontier
About this book
Among neuromodulation procedures, electrical stimulation of peripheral nerves (PNS) is probably the most underappreciated modality. Although PNS is used for all kinds of medical conditions, ranging from chronic neuropathic pain and headache to epilepsy, depression, hypertension and heart failure, its importance is frequently overshadowed by spinal cord stimulation and deep brain stimulation. While the earlier version of this book dealt exclusively with various pain syndromes, this new volume covers the entire spectrum of PNS applications. Written by recognized authorities in their respective fields, the chapters of this title describe the use of PNS in the management of neurological, psychiatric, otorhinolaryngological, cardiovascular, pulmonary, colorectal and genitourinary disorders. To reflect the complexity of the regulatory process, the book ends with a special chapter dedicated to the current state of approval of different PNS devices. This book will be of great value to all those who deal with neuromodulation, including clinicians who select PNS candidates, surgeons and other specialists who implant PNS devices, and researchers and engineers who work on making the stimulators safer and more effective.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Ear, Nose & Throat MedicineSlavin KV (ed): Stimulation of the Peripheral Nervous System. The Neuromodulation Frontier.
Prog Neurol Surg. Basel, Karger, 2016, vol 29, pp 168-191 (DOI: 10.1159/000434670)
Prog Neurol Surg. Basel, Karger, 2016, vol 29, pp 168-191 (DOI: 10.1159/000434670)
______________________
Peripheral Neurostimulation with a Microsize Wireless Stimulator
Thomas L. Yearwooda, b · Laura Tyler Perrymanc
aComprehensive Pain and Rehabilitation, Pascagoula, Miss., bDepartment of Neurology, University of South Alabama, Mobile, Ala., and cStimwave Inc., Fort Lauderdale, Fla., USA
______________________
Abstract
Implementation of wireless technology enables tremendous reduction in the size of implantable neurostimulator devices. Without the need for tethering to an implantable pulse generator, a multitude of clinical applications can be envisioned, utilizing safe, rapidly implanted, economical, and culturally sensitive methods. External pulse generators providing power to implanted microsize wireless leads and/or contact pairs can be incorporated into belts, fabric, jewelry, and other suitable and convenient accoutrements. Microsized wireless neurostimulator lead placements can provide neuromodulation therapies without mechanically compromising normal physiological function in numerous anatomical locations not so accessible now. Avoiding implantation of the pulse generator dramatically reduces the expense of these therapies and can potentially lead to wider global access of care for neuromodulation in general.
© 2016 S. Karger AG, Basel
Brief Overview of Wireless Technology
In 1873, Scottish physicist James Clerk Maxwell was one of the first to describe electromagnetic energy in a series of mathematical relationships incorporating the relationship between light, magnetism, and electricity into a single unified field theory known as the Maxwell equations. This was the first major challenge to Newtonian mechanics and cannot be overestimated in its significance, both philosophically and practically. In the years that followed, the ideas came to fruition when Franz Hertz successfully transferred energy from one device to another using electromagnetic waves. Further developments rapidly ensued, and we now take for granted a life surrounded by myriads of electromagnetic wave generators and receivers used for communication (the transmission of data) and power (the transmission of energy).
Radio frequency radiation (RFR) occurs when a waveform is transmitted through a medium at a frequency within the radio frequency (RF) portion of the electromagnetic spectrum: frequencies from 10 kHz to 300 GHz. The frequency range of RFR includes the most common frequencies used in transmitting data and power to medical devices. In general, electromagnetic waves include magnetic waves and electric waves that synchronously radiate at perpendicular angles to each other (fig. 1).
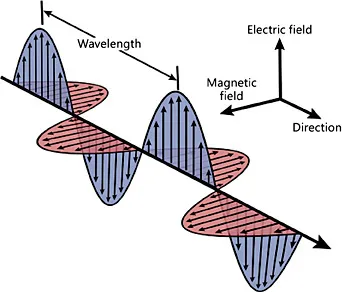
Fig. 1. Three-dimensional representation of the electromagnetic wave: magnetic and electric components of the waveform (modified from http://qph.is.quoracdn.net/main-qimg-5055566df5ba9809b22c262801246760?convert_to_webp=true).
A narrower band of frequencies within the frequency range of RFR, from 100 to 500 kHz, is known as the inductive range. These frequencies tend to be the most efficient at creating an induced current by means of an electromagnetic flux passing across coiled circuits. Frequencies within the inductive range band are most commonly used to charge implanted medical devices. The Medical Implant Communication Services (MICS) band of frequencies from 402 to 405 MHz is specified by governmental agencies to be reserved for communications with medical implants. Uninterrupted communication with medical implants is absolutely essential to the well-being of the patient, which is why the MICS band must be safeguarded carefully. The primary safety concern with using inductive power is the amount of heating which can occur at the tissue interface. Thermal heating is a function of the specific absorption rate, which is the amount of absorbed energy measured in watts per kilogram of tissue (W/kg). Electromagnetic fields used for medical device implant power are classified as near fields, and are typically nonpropagating in nature, vary in strength rapidly over distance from the source, and are subject to interference with objects placed near the source.
With near fields, the trade-off for transmission power from the source is typically a balance between specific absorption rate, range of distance from the source of power (emitter) to coiled antenna (receiver), and power consumption. It should be noted it is a critical requirement for near-field power and communications transmission to maintain appropriate alignment of the emitting and receiving devices. As alignment of the emitter and receiver is varied, the efficiencies of power and communications transfer are altered, reaching a minimum at a 90° offset in any combination of three-dimensional space. The clinical importance of maintaining appropriate alignment governs the size, shape, and anatomic location of remotely powered implantable medical devices. In the inductive range, a more shallow location is needed for the receiver coils.
Table 1. Sensations associated with dermal and subdermal sensory fibers (modified from Verrills and Barnard [12])
Fiber types | Associated sensation |
A-β: fast adapt | Tingling, tickling |
A-β: slow adapt | Vibrating |
A-δ | Sharp pain, stinging |
C fibers | Burning, aching |
Dermis: mostly A-δ. Subcutaneous tissue: more A-β. Optimal depth below dermal surface for A-β fast adapt: 10-12 mm. | |
In this chapter we discuss various types of pulse generators that have been used in neurostimulation in order to understand the evolution that has led to the development of wireless pulse generators (WPGs) and their clinical applications.
Fundamentals of Neurostimulation Technology
External Pulse Generators
Transcutaneous Electrical Nerve Stimulation
Transcutaneous electrical nerve stimulation units are commonly used to elicit an electric field on the surface of the dermis in order to recruit sensory nerve fibers and muscle fibers near the electrodes. The dermis itself is particularly rich in unmyelinated C-nociceptive sensory fibers, with a variable population density of A-δ sensory nerves at certain locations. Deep to the dermis, in the subcutaneous fat between the dermis and the first fascial layer, there are numerous A-β sensory nerve fibers. Muscle fiber recruitment begins within the first fascial layer. Depending on the distance from the dermis to the first fascial layer, the intensity of the stimulation may be such that recruitment of the C-nociceptive unmyelinated fibers and the A-δ fibers becomes quite uncomfortable if a motor response is clinically indicated for this therapy. Table 1 demonstrates the typical human sensory perception for each of these different neuronal recruitments.
Transcutaneous electrical nerve stimulation is the most commonly used form of electroanalgesia, primarily due to the noninvasive nature of the therapy and its associated cost (‘price point’). A transcutaneous electrical nerve stimulation device typically consists of externally placed electrode pads, from as few as 2 to 12 or more, wired to an external battery-powered electrical signal generator carried with the patient. This signal generator creates a biphasic waveform electric field with pulse widths from 10 to 1,000 µs (typically 50 µs), pulse rates (frequency) from 1 to 150 Hz, and at amplitudes of 10 to 30 mA. Skin irritation can occur in many patients from electrode adhesives or improperly applied electrode gel.

Fig. 2. Radiofrequency pulse generator. Note the presence of coils to convert power externally through the dermis by means of electromagnetic coupling using frequencies in the induction range.
Radiofrequency Pulse Generator
Radiofrequency pulse generators (RPGs) are pulse generators powered by inductively coupled energy from outside the body. These devices contain a coil receiver (fig. 2), which receives power from an external pulse generator (EPG). Using RFR in the inductive range of frequencies, power is transferred through the dermis and subcutaneous tissues to the implanted RPG. The energy produced within the RPG receiver coils is routed to microelectronic circuitry, which generates a biphasic waveform pulse. This biphasic waveform pulse is then routed to a connector attached to a wired lead containing 4-8 individual electrode contacts, depending on the anatomy of the targeted neuronal pathways.
The RPG system has advantages and disadvantages for durable neurostimulation therapy. The potential advantage is a theoretical ability to upgrade the system software, and possibly even the firmware, without explanting part or all of the system, as advanced programming paradigms may become available. There is also an ease of changing or recharging the battery of an external RPG rather than replacing or recharging the implanted generator. The primary disadvantages of the RPG are concerns reg...
Table of contents
- Cover Page
- Front Matter
- Technology for Peripheral Nerve Stimulation
- Theoretical Basis of Vagus Nerve Stimulation
- Vagus Nerve Stimulation: Surgical Technique and Complications
- Vagus Nerve Stimulation for Epilepsy: An Evidence-Based Approach
- Vagus Nerve Stimulation for Major Depressive Episodes
- Phrenic Nerve Stimulation: Technology and Clinical Applications
- Trigeminal Ganglion Stimulation
- Carotid Sinus/Nerve Stimulation for Treatment of Resistant Hypertension and Heart Failure
- Hypoglossal Nerve Stimulation for Obstructive Sleep Apnea
- Sphenopalatine Ganglion Stimulation in Neurovascular Headaches
- Occipital Nerve Stimulation for Migraine: Update from Recent Multicenter Trials
- Peripheral Nerve Stimulation for Back Pain
- Peripheral Nerve Stimulation for Pain in Extremities: An Update
- Peripheral Neuromodulation to Treat Postamputation Pain
- Peripheral Neurostimulation with a Microsize Wireless Stimulator
- Sacral Neuromodulation for Genitourinary Problems
- Sacral Nerve Stimulation in the Treatment of Bowel Disorders
- Stimulation of the Dorsal Root Ganglion
- Regulation of Peripheral Nerve Stimulation Technology
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Stimulation of the Peripheral Nervous System by K. V. Slavin,K.V., Slavin, K. V. Slavin,Konstantin V. Slavin,Konstantin V., Slavin in PDF and/or ePUB format, as well as other popular books in Medicine & Ear, Nose & Throat Medicine. We have over 1.5 million books available in our catalogue for you to explore.