Comparative Cardiac Imaging
A Case-based Guide
- English
- ePUB (mobile friendly)
- Available on iOS & Android
Comparative Cardiac Imaging
A Case-based Guide
About this book
Provides the information necessary to guide clinicians to more efficient and appropriate use of the cardiac imaging modalities at their disposal
Most books currently available on cardiac imaging focus on just modality. As the number of imaging options has increased, the choice of procedure has become more complicated. This comprehensive book will guide the practitioner in choosing the most appropriate test when confronted by various cardiac symptoms and diseases and to understand the benefits and limitations of each imaging modality. It demonstrates the advantages and disadvantages of various imaging modalities such as echocardiography, computer tomography, MRI, and nuclear cardiology in the evaluation of various disease states both commonly and infrequently seen in a standard practice.
Comparative Cardiac Imaging—A Case-based Guide utilizes actual case examples to demonstrate the state of the art in comparative cardiac imaging. It offers in-depth chapter coverage of Aortic Diseases; Aortic Valvular Diseases; Mitral Valvular Diseases; Prosthetic Valves; Coronary Artery Disease; Pulmonary Artery Diseases; Congenital Heart Disease; Cardiac Tumor; Infective Disease; Cardiomypathy; and Cardiac Trauma.
- Uniquely focuses on and compares the many different modalities for cardiac imaging
- Breaks the topic down by anatomy and pathophysiology in order to cover all aspects of non-invasive cardiac imaging
- Covers newer and lesser known modalities like speckle tracking and velocity vector imaging
- Offers coverage of more controversial topics, such as CT angiography
Comparative Cardiac Imaging—A Case-based Guide presents a level of data that is appropriate for the practicing cardiologist and cardiology trainee, as well as residents, internists, and other primary care clinicians.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Part I
Congenital Heart Disease in the Adult
1
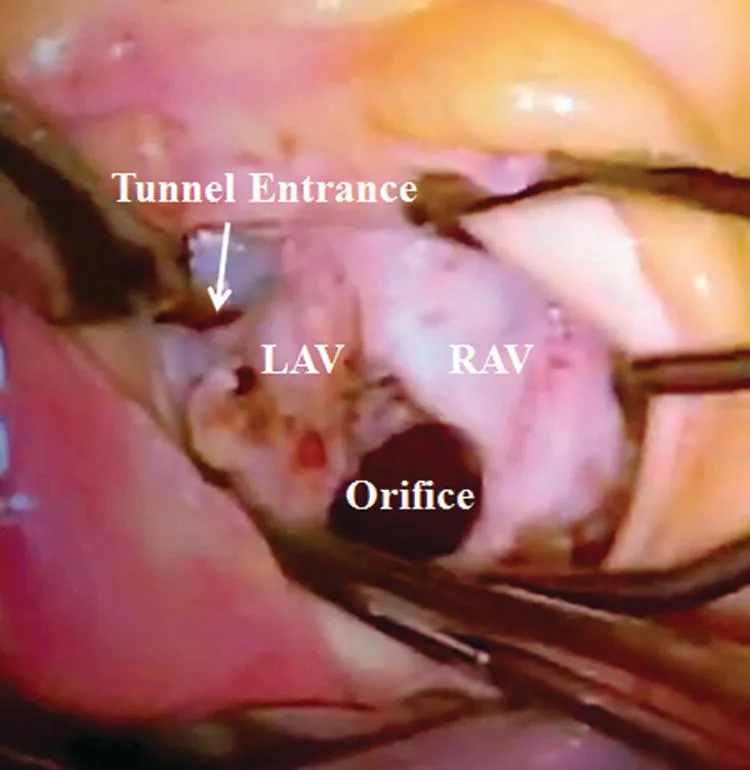
Aneurysmal Aorto–Left Ventricular Tunnel and Bicuspid Aortic Valve with Severe Stenosis
History
Physical Examination
Transthoracic Echocardiogram



Management
Discussion
Associated Anomalies
Clinical Presentation
Table of contents
- Cover
- Title Page
- Table of Contents
- Notes on Contributors
- Foreword
- Preface
- Abbreviations
- About the Companion Website
- Part I: Congenital Heart Disease in the Adult
- Part II: Artery Disease
- Part III: Cardiac Mass
- Part IV: Cardiomyopathy and Myocarditis
- Part V: Diversification
- Index
- End User License Agreement
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app