Salivary Gland Pathology: Diagnosis and Management, Second Edition, updates the landmark text in this important discipline within oral and maxillofacial surgery, otolaryngology/head and neck surgery, and general surgery. Written by well-established clinicians, educators, and researchers in oral and maxillofacial surgery, this book brings together information on the etiology, diagnosis, and treatment of all types of salivary gland pathology. Clear and comprehensive, Salivary Gland Pathology: Diagnosis and Management offers complete explanation of all points, supported by a wealth of clinical and surgical illustrations to allow the reader to gain insight into every facet of each pathologic entity and its diagnosis and treatment.
Salivary Gland Pathology: Diagnosis and Management offers comprehensive coverage of all aspects of this topic. Beginning with the embryology, anatomy and physiology of the salivary glands, the first section of the book discusses radiographic imaging, infections, cystic conditions, sialoadenitis and sialolithiasis, and systemic diseases. The second section of the book is devoted to the classification of salivary gland tumors and devotes individual chapters to the discussion of each type. Additions for this section of the second edition include molecular biology of salivary gland neoplasia, radiation therapy, and chemotherapy and targeted therapy for salivary gland malignancies. The book closes with a discussion of pediatric salivary gland pathology, traumatic injuries of the salivary glands and miscellaneous pathologic processes of the salivary glands and ducts, including a section on saliva as a diagnostic fluid.
The book is intended for a very diverse audience, including academic oral and maxillofacial surgeons, otolaryngologists / head and neck surgeons, general surgeons, as well as residents in these disciplines. Private practitioners will want to place this publication on the bookshelves of their offices so as to consult the textbook when evaluating a patient with salivary gland pathology.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands
John D. Langdon, FKC, MB BS, BDS, MDS, FDSRCS, FRCS, FMedSci
Outline
- Introduction
- The Parotid Gland
- Embryology
- Anatomy
- Contents of the Parotid Gland
- The Facial Nerve
- Auriculotemporal Nerve
- Retromandibular Vein
- External Carotid Artery
- Parotid Lymph Nodes
- Parotid Duct
- Nerve Supply to the Parotid
- The Submandibular Gland
- Embryology
- Anatomy
- The Superficial Lobe
- The Deep Lobe
- The Submandibular Duct
- Blood Supply and Lymphatic Drainage
- Nerve Supply to the Submandibular Gland
- Parasympathetic Innervation
- Sympathetic Innervation
- Sensory Innervation
- The Sublingual Gland
- Embryology
- Anatomy
- Sublingual Ducts
- Blood Supply, Innervation, and Lymphatic Drainage
- Minor Salivary Glands
- Histology of the Salivary Glands
- Control of Salivation
- Summary
- References
Introduction
There are three pairs of major salivary glands consisting of the parotid, submandibular, and sublingual glands. In addition, there are numerous minor glands distributed throughout the oral cavity within the mucosa and submucosa.
On average, about 0.5 liters of saliva are produced each day but the rate varies throughout the day. At rest, about 0.3 ml/min are produced but this rises to 2.0 ml/min with stimulation. The contribution from each gland also varies. At rest, the parotid produces 20%, the submandibular gland 65%, and the sublingual and minor glands 15%. On stimulation, the parotid secretion rises to 50%. The nature of the secretion also varies from gland to gland. Parotid secretions are almost exclusively serous, the submandibular secretions are mixed and the sublingual and minor gland secretions are predominantly mucinous.
Saliva is essential for mucosal lubrication, speech, and swallowing. It also performs an essential buffering role that influences demineralization of teeth as part of the carious process. When there is a marked deficiency in saliva production, xerostomia, rampant caries, and destructive periodontal disease ensues. Various digestive enzymes – salivary amylase – and antimicrobial agents – IgA, lysozyme, and lactoferrin – are also secreted with the saliva.
The Parotid Gland
Embryology
The parotid gland develops as a thickening of the epithelium in the cheek of the oral cavity in the 15 mm Crown Rump length embryo. This thickening extends backwards towards the ear in a plane superficial to the developing facial nerve. The deep aspect of the developing parotid gland produces bud like projections between the branches of the facial nerve in the third month of intra-uterine life. These projections then merge to form the deep lobe of the parotid gland. By the sixth month of intra-uterine life the gland is completely canalized. Although not embryologically a bilobed structure, the parotid comes to form a larger (80%) superficial lobe and a smaller (20%) deep lobe joined by an isthmus between the two major divisions of the facial nerve. The branches of the nerve lie between these lobes invested in loose connective tissue. This observation is vital in the understanding of the anatomy of the facial nerve and surgery in this region (Berkovitz, et al. 2003).
Anatomy
The parotid is the largest of the major salivary glands. It is a compound, tubuloacinar, merocrine, exocrine gland. In the adult, the gland is composed entirely of serous acini.
The gland is situated in the space between the posterior border of the mandibular ramus and the mastoid process of the temporal bone. The external acoustic meatus and the glenoid fossa lie above together with the zygomatic process of the temporal bone (Figure 1.1). On its deep (medial) aspect lies the styloid process of the temporal bone. Inferiorly, the parotid frequently overlaps the angle of the mandible and its deep surface overlies the transverse process of the atlas vertebra.
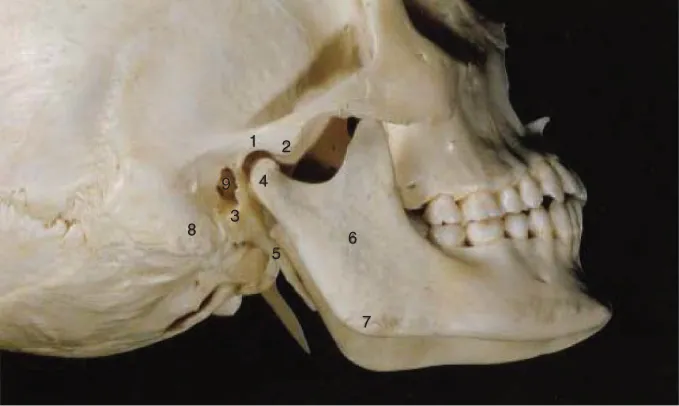
Figure 1.1 A lateral view of the skull showing some of the bony features related to the bed of the parotid gland. 1: Mandibular fossa; 2: Articular eminence; 3: Tympanic plate; 4: Mandibular condyle; 5: Styloid process; 6: Ramus of mandible; 7: Angle of mandible; 8: Mastoid process; 9: External acoustic meatus. Source: Surgical Management of the Infratemporal Fossa. (J. Langdon, B. Berkovitz & B. Moxham). ISBN 9781899066797. Reproduced with permission of Taylor & Francis Books UK.
The shape of the parotid gland is variable. Often it is triangular with the apex directed inferiorly. However, on occasion it is more or less of even width and occasionally it is triangular with the apex superiorly. On average, the gland is 6 cm in length with a maximum of 3.3 cm in width. In 20% of subjects a smaller accessory lobe arises from the upper border of the parotid duct approximately 6 mm in front of the main gland. This accessory lobe overlies the zygomatic arch.
The gland is surrounded by a fibrous capsule previously thought to be formed from the investing layer of deep cervical fascia. This fascia passes up from the neck and was thought to split to enclose the gland. The deep layer is attached to the mandible and the temporal bone at the tympanic plate and styloid and mastoid processes (McMinn, et al. 1984; Berkovitz and Moxham 1988; Williams 1995; Ellis 1997). Recent investigations suggest that the superficial layer of the parotid capsule is not formed in this way, but is part of the superficial musculo-aponeurotic system (SMAS) (Mitz and Peyronie 1976; Jost and Levet 1983; Wassef 1987; Thaller, et al. 1989; Zigiotti, et al. 1991; Gosain, et al. 1993; Flatau and Mills 1995). Anteriorly, the superficial layer of the parotid capsule is thick and fibrous but more posteriorly, it becomes a thin translucent membrane. Within this fascia are scant muscle fibers running parallel with those of the platysma. This superficial layer of the parotid capsule appears to be continuous with the fascia overlying the platysma muscle. Anteriorly, it forms a separate layer overlying the masseteric fascia, which is itself an extension of the deep cervical fascia. The peripheral branches of the facial nerve and the parotid duct lie within a loose cellular layer between these two sheets of fascia. This observation is important in parotid surgery. When operating on the parotid gland, the skin flap can either be raised in the subcutaneous fat layer or deep to the SMAS layer. The SMAS layer itself can be mobilized as a separate flap and can be used to mask the cosmetic defect following parotidectomy by reattaching it firmly to the anterior border of the sternocleidomastoid muscle as an advancement flap (Meningaud, et a...
Table of contents
- Cover
- Title Page
- Copyright
- Table of Contents
- Contributors
- Foreword First Edition
- Foreword Second Edition
- Preface First Edition
- Preface Second Edition
- Acknowledgments
- Chapter 1: Surgical Anatomy, Embryology, and Physiology of the Salivary Glands
- Chapter 2: Diagnostic Imaging of Salivary Gland Pathology
- Chapter 3: Infections of the Salivary Glands
- Chapter 4: Cysts and Cyst-like Lesions of the Salivary Glands
- Chapter 5: Sialolithiasis
- Chapter 6: Systemic Diseases Affecting the Salivary Glands
- Chapter 7: Classification, Grading, and Staging of Salivary Gland Tumors
- Chapter 8: The Molecular Biology of Benign and Malignant Salivary Gland Tumors
- Chapter 9: Tumors of the Parotid Gland
- Chapter 10: Tumors of the Submandibular and Sublingual Glands
- Chapter 11: Minor Salivary Gland Tumors
- Chapter 12: Radiation Therapy for Salivary Gland Tumors
- Chapter 13: Systemic Therapy for Salivary Gland Cancer
- Chapter 14: Non-salivary Tumors of the Salivary Glands
- Chapter 15: Pediatric Salivary Gland Pathology
- Chapter 16: Trauma and Injuries to the Salivary Glands
- Chapter 17: Miscellaneous Pathologic Processes of the Salivary Glands
- Index
- End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Salivary Gland Pathology by Eric R. Carlson,Robert A. Ord in PDF and/or ePUB format, as well as other popular books in Médecine & Chirurgie et médecine chirurgicale. We have over 1.5 million books available in our catalogue for you to explore.