![]()
Part 1:Basic Principles
Section Editor. Tony Pogrel
1 Patient Evaluation
Alan S. Herford and Wayne K. Tanaka
2 Radiographic Imaging in Oral and Maxillofacial Surgery
Arne Petersson
3 Medical Aspects - High-risk Patients
Earl G. Freymiller
4 Medical Emergency Care
Zachary S. Peacock and M. Anthony Pogrel
5 Local Anesthesia
John Gerard Meechan
6a Sedation and General Anesthesia in Oral and Maxillofacial Surgery: A UK Perspective
C. Michael Hill
6b Sedation and General Anesthesia in Oral and Maxillofacial Surgery: A US Perspective
Richard C. Robert
7 Dentofacial Infection
Ashraf Ayoub
8 Armamentarium for Basic Procedures
Ala Al-Musawi
9 Basic Surgical Principles
M. Anthony Pogrel and Fabio Kricheldorf
10 Complications Associated with Dentoalveolar Surgery
Srinivas M. Susarla, Ryan J. Smart, and Thomas B. Dodson
11a Normal Wound Healing
Anh Le and Vivek Shetty
11b Compromised Wound Healing
Gösta Granström
![]()
Chapter 1
Patient Evaluation
Alan S. Herford and Wayne K. Tanaka
This chapter will cover how to obtain a patient history and carry out a full physical examination. It will cover comorbidities and systemic diseases of relevance to the oral and maxillofacial surgeon in the cardiovascular system (including cardiac disease and hypertension), the pulmonary system (including tobacco use and asthma), and also the endocrine systems, to cover obesity.
Suitable imaging and laboratory studies will also be discussed to arrive at a diagnosis of the patient’s medical history, assess anesthetic and surgical risks, and determine whether a procedure would be best carried out in the office or as an inpatient taking into account the medical history.
Obtaining a patient history
Physical examination
Comorbidities/systemic diseases
Cardiovascular system
Pulmonary system
Endocrine system
Obesity
Other organ systems
Imaging
Laboratory studies
Arriving at a diagnosis
Assessing anesthetic/surgical risk
Office vs inpatient
Summary
The goal of preoperative evaluation is to reduce patient risk and the morbidity of surgery and is based on the premise that it will modify patient care and improve outcome. The preoperative evaluation has several components and should be guided by the patient and surgery being contemplated. It is important to understand that some patients will require an in-depth, thorough examination prior to undergoing surgery, whereas others may benefit from a more focused examination. The type depends on many factors including the age and health of the patient, existing comorbidities, and the type of surgical procedure planned. Thus, it is important for the clinician to understand how to perform a detailed, in-depth history and physical examination.
The Joint Commission for the Accreditation of Healthcare Organizations (JCAHO) requires that all patients receive a preoperative anesthetic evaluation and the American Society of Anesthesiologists (ASA) has approved Basic Standards for Preoperative Care which outline the minimum requirements for a preoperative evaluation. Preoperative patient assessment is important in order to develop a safe and appropriate surgical and anesthetic plan.1–11 During the preoperative assessment the clinician interviews either the patient or knowledgeable guardian to obtain information. This is followed by a physical examination with special emphasis on the cardiovascular and respiratory systems to help determine risk. Laboratory tests, imaging, and consultations are ordered as deemed necessary based on information obtained during the history and physical examination. Finally, diagnoses are formulated and the treatment options are discussed with the patient followed by obtaining an informed consent.
Obtaining a patient history
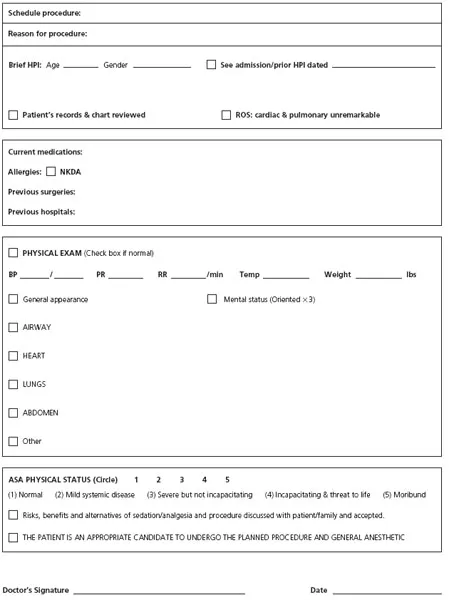
The importance of an accurate, detailed history cannot be overemphasized because it provides the framework on which the clinician builds an accurate diagnosis and treatment plan (Fig. 1.1) An inaccurate or incomplete evaluation may lead to a delay in treatment, unnecessary testing, or misdiagnosis.
It is often helpful to review previous medical records. This can provide important information and save time during the interview process. Information such as medications and doses and history of previous surgeries are some examples that can be gleaned from the previous medical records. The clinician may uncover a history of a difficult airway or a history of malignant hyperthermia, and the patient’s response to surgical stress and specific anesthetics may be evaluated. If the patient presents in an altered state, these records can be especially helpful. Preoperative questionnaires and computer-driven programs are becoming more common as a way to gather information and save time. This should help to alert the clinician on areas to focus on but should not be used as an alternative to interviewing the patient.
The clinician must assess the reliability of the person giving the history. Every patient should be asked about their chief complaint (CC). This should be transcribed into the medical record in the patient’s own words. The chief complaint assists the clinician in establishing priorities during the history-taking process.
The patient should be asked to describe the history of the present illness (HPI). Information should be gathered regarding onset, intensity, quality, location, duration, radiation, and any exacerbating or relieving factors. Constitutional symptoms that relate to the present illness should also be noted. Examples of pertinent positives and negatives with regard to the chief complaint may include fever, chills, loss of weight, weakness, etc.
The past medical history (PMH) alerts the clinician to any coexisting illnesses that may have an impact on any planned surgeries. Information regarding the severity of an illness should be obtained. For example if a patient reports a history of asthma, the severity and frequency of episodes, previous hospital treatments, and current control should be ascertained. Past surgical history can also help to identify factors that may impact the ability for a patient to undergo a safe surgical procedure. Patients should be asked about medications they are taking as well as any over-the-counter and herbal products. Any allergies to drugs should also be documented, including what type of allergic response a patient may have experienced. A family history (FH) may reveal risk factors for patients as well as the possibility of inherited illnesses such as hemophilia or malignant hyperthermia.
The social history (SH) of a patient should include information regarding their social support system and also any habits such as tobacco, alcohol, or illicit drug use. These habits may adversely affect healing and also increase a patient’s risk for undergoing a planned surgical procedure.
A review of systems (ROS) is a comprehensive method of inquiring about a patient’s symptoms on an organ system basis. The review of systems may reveal undiagnosed medical conditions unknown to the patient. Concerns raised in the cardiovascular and respiratory systems for example may have importance with regard to a patient undergoing a safe surgical procedure. Patients should also be asked about the presence or recent history of an upper respiratory infection. Symptoms such as shortness of breath, cough, wheezing, stridor, snoring, or sleep apnea can alert the clinician to underlying illness that may increase the risk of morbidity associated with a procedure.
Physical examination
During the physical exam the clinician further reinforces or disproves impressions gained during the history-taking portion. Vital signs are recorded at the beginning of the physical exam. These include blood pressure, pulse rate, respiratory rate, and temperature. Next the patient’s general appearance should be noted. It is important when documenting findings to only use commonly used, accepted abbreviations in order to avoid confusion. The physical exam should proceed in a stepwise, systematic manner. Evaluation typically involves inspection, palpation, percussion, and auscultation of the organ system being evaluated. The areas involved typically include the head, eyes, ears, nose, and throat (HEENT) region, in addition to the lungs, abdomen, heart, genitourinary, musculo-skeletal, skin, and neurological exam. The detail in which these examinations take place is based on the health of the patient, including any comorbidities, and the type of surgical procedure planned. The examination may be cursory in healthy patients or extensive in patients with coexisting disease. For patients sustaining severe trauma a neurological examination should include a Glasgow Coma Score (Table 1.1). A cranial nerve exam should be performed to uncover any abnormalities (Table 1.2). For patients undergoing facial trauma, the eyes should be evaluated for any afferent pupillary light defects (Fig. 1.2).
Table 1.1 Glascow coma scale.
| EYE RESPONSE (E) |
| 4 = Open spontaneously |
| 3 = Open to verbal command |
| 2 = Open to pain |
| 1 = No response |
| VERBAL RESPONSE (V) |
| 5 = Oriented, converses |
| 4 = Disoriented, converses |
| 3 = Inappropriate responses |
| 2 = Incomprehensible |
| 1 = No response |
| MOTOR RESPONSE (M) |
| 6 = Obeys verbal command |
| 5 = Localizes to pain |
| 4 = Withdrawal from pain |
| 3 = Decorticate (flex) to pain |
| 2 = Decerebrate (extend) to pain |
| 1 = No... |