![]()
1
THE RADIOGRAPHS AND ANATOMY OF THE CHEST X-RAY
Posterior anterior x-rays
The chest x-ray is normally taken PA (posterior anterior) standing, when the patient’s condition permits, at a distance of 180cm, the scapula rotated away from the lungs, centred at thoracic vertebra 4 (T4) on full inspiration (as demonstrated below). However, some centres suggest centring at T4, then angling the x-ray tube to T6 to avoid irradiating the sensitive eyes. X-raying the chest PA and at 180cm reduces magnification of the heart. Removing the scapula from the lungs avoids misinterpretation of the overlying scapula as pathology. It also allows clear visualisation of the lungs. Poor inspiration will make the heart look larger, and may give the appearance of basal shadowing and cause the trachea to appear deviated to the right. If the patient is standing, it is easier for them to take a deep breath in.
When reviewing the chest image, the first thing to check (before the anatomy or anything else) is whether the correct patient has been x-rayed on the correct date. Having checked these details, you can then assess the quality of the image, as this may affect your final interpretation.
Table 1.1: Quality issues
| Issue |
| PA, AP, sitting or supine | This will affect magnification/heart size |
| Rotation | Medial ends of clavicles should be equidistant from spinous process of vertebra |
| Lordotic/kyphotic | Clavicles should be posterior end of 4th rib, not above or below |
| Scapula removed from lungs | If not, be careful with interpretation |
| Full inspiration | Inspired to 5–6.5 anterior ribs, or 10/11 posterior ribs |
| Entire lungs included on image | If not, repeat may be required |
| Artefacts | Beware that an artefact is not misinterpreted as pathology |
| Correct marker/annotations | Is the patient really dextracardia? |
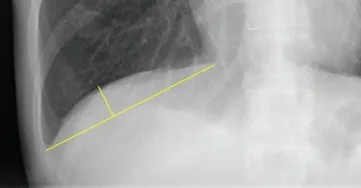
If assessing inspiration, we first need to know which ribs we are counting – anterior or posterior. The above image demonstrates this. In certain conditions the lungs will be hyperventilated, and more than 11 posterior ribs will be visualised. In emphysema, the lungs may be so hyper-inflated that the diaphragm is flattened. The height of the diaphragm should normally be 1.5cm (see Figure 1.4, which shows how the diaphragm is measured).
If the patient is rotated, this will affect how the mediastinum is projected. Rotation to the right on a PA chest x-ray will result in the superior vena cava and/or other vessels arising from the arch of the aorta becoming more prominent. Severe rotation may result in one lung appearing darker than the other, giving a false impression of some underlying pathology.
A lordotic chest x-ray makes it difficult to accurately assess the pathology of the bases next to the diaphragm. The bases may become ill defined, mimicking pathology, and/or abdominal structures may be projected over the diaphragm and bases. A kyphotic image is most often produced when the patient is kyphotic due to vertebral collapse.
Obtaining a perfect-quality chest x-ray is difficult and the patient’s condition may sometimes make it impossible. You will therefore often have to review a less than perfect-quality chest x-ray. Do this with caution, remembering the effects that rotation, poor inspiration and other factors may have on the final image. In most cases, it is still possible to answer the clinical question. However, if you have any doubt, a repeat x-ray (often when the patient is more able to cooperate), a lateral view (if possible), or further imaging may be required.
The patient’s condition may often prohibit a PA image. In this case, the patient may have to be x-rayed anterior posterior (AP) in a chair, trolley or bed, or even supine. This will result in increased magnification of the heart and mediastinal structures. An AP sitting image is still taken at a distance of 180cm. However, a supine image is often taken at much less – around 140–120 cm, depending on the x-ray equipment, and how low the trolley or bed can go.
The AP sitting image may be lordotic. If so, take this into consideration when reviewing. Remember also, with a supine patient, fluid within the lungs will tend to sink to the posterior lungs, whereas air will rise. Likewise, effusions and a pneumothorax will appear differently in a supine patient compared to an erect patient (for more on this, see pp. 51–2). In both patient types, increased magnification makes it difficult to accurately assess the mediastinum.
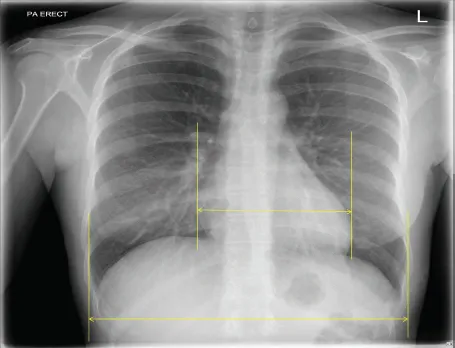
The cardiothoracic ratio (CTR) in a PA patient is normally 50%, whereas on an AP sitting or supine image 60% is a good guideline. Please see Figure 1.7 for guidance on measuring CTR.
PA/AP/supine x-rays
Now we move on to the anatomy demonstrated on a PA/AP/supine chest x-ray. The basic...