![]()
1
ADOLESCENT DEVELOPMENT AND PSYCHOPATHOLOGY
The development of the Minnesota Multiphasic Personality Inventory-Adolescent (MMPI-A) and, most recently, the Minnesota Multiphasic Personality Inventory-Adolescent-Restructured Form (MMPI-A-RF) have substantially assisted in deriving interpretive comments relevant to and appropriate for adolescents, but using these specialized forms of the MMPI does not substitute for an awareness of salient developmental issues. Thus, the purpose of this chapter is to provide a brief overview of adolescent development and psychopathology, with particular attention focused on ways in which developmentally related issues may affect MMPI-A and MMPI-A-RF interpretation practices.
Developmental Tasks During Adolescence
Achenbach (1978) suggested that an understanding of psychopathology in children and adolescents must be firmly grounded in the study of normal development. Human development is a continuous process, but there may be critical periods in our development during which adaptational success or failure heavily influences the course of later development in the life cycle. Adolescence clearly is one of these critical developmental transitions. Holmbeck and Updegrove (1995) have observed that adolescence is “characterized by more biological, psychological, and social role changes than other life stages except infancy” (p. 16). As noted by Petersen and Hamburg (1986), the number and extent of changes that occur simultaneously during adolescence present major challenges to the development of mature and effective coping strategies. Ineffective coping strategies may contribute to a variety of problem behaviors during adolescent development. Further, failures in adolescent development may result in psychopathology manifested during later life stages.
Three major areas of changes and challenges that face the individual during adolescence are reviewed here, including physiological processes, cognitive processes, and psychological and emotional challenges.
Physiological/Sexual Maturation
Kimmel and Weiner (1985) defined puberty as “the process of becoming physically and sexually mature and developing the adult characteristics of one’s sex” (p. 592). Petersen (1985) noted several characteristics of puberty that are important in understanding adolescent development. Puberty is a universal experience that may, however, be delayed, or in some cases even prevented by the occurrence of physical disease or traumatic psychological events. Paikoff and Brooks-Gunn (1991) noted that the timing of puberty has been shown to vary as a function of the adolescent’s health status, nutrition, ethnicity, genetic inheritance, exercise level, and stress experiences. They observed that the parent–child relationship is typically affected by pubertal development, with decreases in time spent with parents and submissiveness to parental decisions typically found during early adolescence. Further, Petersen stressed that puberty is a process, rather than an isolated temporal event. This process involves changes that result in a sexually immature child achieving full reproductive potential. These physical changes are typically manifested in the growth of underarm and pubic hair, maturation of genitalia, and the first menstruation in girls. Often, the clearest signs of adolescent development are physical changes associated with the onset of puberty.
Fundamental physical changes, in terms of endocrinological, biochemical, and physiological processes, occur during adolescence. For example, Stone and Church (1957) noted that an individual is expected to increase 25% in height and 100% in weight during this developmental stage. Additionally, there is a marked increase in pituitary activity leading to increased production of hormones by the thyroid, adrenal, and other glands that are centrally involved in sexual maturation.
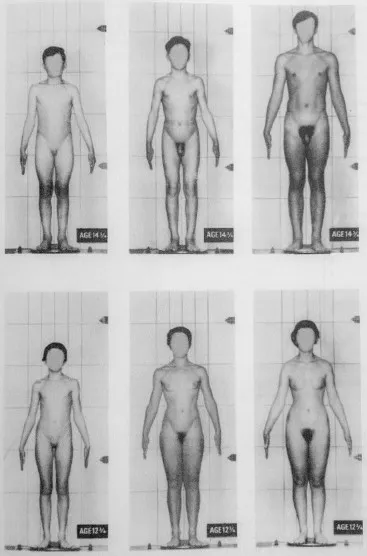
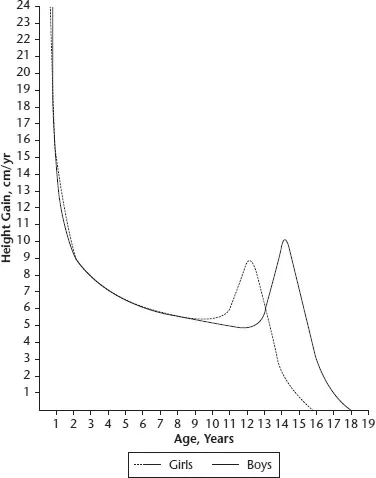
There are notable differences in the rate of physical maturation between boys and girls, and there are also very wide individual variations in sexual maturation within genders. Figures 1.1 and 1.2 show varying degrees of sexual maturation for boys aged 143/4 and girls aged 123/4, and the velocity of growth in height by year of life. The data in Fig. 1.1 for pubertal development illustrate both the earlier maturation of females in relation to males, and the wide differences in pubertal development within genders at identical chronological ages. To the extent that pubertal development is precocious or significantly delayed, stress may occur that can be reflected in lower self-esteem or self-concept for the adolescent during this period. A monograph by the American Psychological Association (APA, 2002) provided data indicating that the current course of pubertal development for American adolescents is occurring substantially earlier than the guideposts originally provided by Tanner in the late 1960s for his British sample of adolescents. For example, the average age of menarche for girls in the United States is now around 12.5, and for boys the onset of puberty involving the enlargement of the testes occurs at around age 11.5, with the first ejaculation typically occurring between the ages of 12 and 14. A survey of 17,000 healthy girls between the ages of 3 and 12 who were participating in office visits with their pediatricians found that 6.7% of White girls and 27.2% of African-American girls showed some signs of puberty as early as age 7, e.g., pubic hair or breast development (Herman-Giddens et al., 1997; Kaplowitz & Oberfield, 1999). A description of the adolescent growth spurt by Hoffmann and Greydanus (1997) is generally consistent with the earlier data by Tanner in indicating that the rapid skeletal developments which mark the growth spurt usually begin at around ages 10 to 12 in girls and around ages 12 to 14 for boys. The most dramatic rate of physical growth, shown in Fig. 1.2, tends to occur between the ages of 12 and 15, with the peak of the growth curve occurring approximately two years earlier for females than for males.
An illustration of the influence of developmental forces on MMPI responses is provided by the item, “I worry about sex.” This item is endorsed in the true direction by 13% of adult female respondents in the MMPI-2 normative sample (Butcher, Dahlstrom, Graham, Tellegen and Kaemmer, 1989), and 15% of adult men. In contrast to adult samples, however, this item was endorsed as true by 37% of adolescent females and 30% of adolescent males in the MMPI-A normative sample (Butcher et al. 1992). The higher rate of endorsement of this item in the critical direction by the 14- to 18-year-old teenagers probably reflects the higher level of stress for adolescents related to issues of sexual maturation as well as sexual identity.
Cognitive Maturation and Brain Development
Adolescence may also be defined in terms of changes that occur in cognitive processes and brain development. White (2009) recently observed that as the adolescent begins the physical changes associated with puberty, the brain also undergoes dramatic changes with profound implications for development and psychopathology. White notes that some of the most intriguing of these changes occur in the frontal lobe area of the brain, a region associated with critical roles in decision-making and higher-order cognitive functioning. Frontal lobe gray matter volume reaches a peak around age 11 for girls and 12 for boys, at which point the brain begins the process of reducing brain volume and “pruning” synaptic connections into a configuration that will carry the individual through the adult years. These changes occurring in the frontal lobes during adolescence reflect a refinement of brain circuitry allowing for increased efficiency of functioning. Albert, Chein, and Steinberg (2013) have noted research findings that suggest that adolescent risk-taking behaviors derive, at least in part, from the maturational gap that occurs during early adolescence in terms of brain development. As the cognitive control system of the brain matures over the period of adolescence, teenagers grow correspondingly in their capacity to inhibit risk-taking and exercise self-regulation and control. Bonnie and Scott (2013) have noted that neuroscience has played an increasingly important role in juvenile justice policy concerning questions of whether and when adolescent offenders should be punished as adults. They noted three recent court opinions emphasizing reduced culpability of adolescents because of developmental immaturities, in part supported by neuroscience research. These decisions include Roper v. Simmons (2005) in which the Supreme Court rejected the death penalty for adolescents, and Graham v. Florida (2010) and Miller v. Alabama (2012) which rejected life sentences without parole for juveniles, based heavily on neuroscience research on the role of brain development on behavioral control.
The work of Piaget and his colleagues offers an approach to understanding these cognitive changes, with the final stage of cognitive development in Piaget’s (1975) paradigm unfolding during adolescence. Specifically, Piaget postulated that during early adolescence, the individual typically makes the transition from Concrete Operations to the Formal Operations stage, the latter characterized by the capacity to manipulate ideas and concepts. According to Piaget (1975), “The adolescent is an individual who is capable . . . of building and understanding ideas or abstract theories and concepts. The child does not build theories” (p. 105). Thus, the adolescent is able to discern the real from the ideal, and to become passionately engaged by abstract concepts and notions. Adolescents begin to think of their world in new ways, including the ability to “think about thinking.” Related to these changes in cognitive skills, Elkind (1978, 1980) argued that as adolescents become capable of thinking about their thoughts, they may also become excessively concerned with how they are perceived by others. This preoccupation includes an exaggerated view of the uniqueness of their own experiences, and the amount of time devoted by others to their appraisal. Elkind labeled the egocentric tendency of adolescents to believe that their behavior is intensely scrutinized by others as “the imaginary audience” (Elkind & Bowen, 1979).
Part of this self-absorption and belief in the uniqueness of one’s own experiences may be reflected in the endorsement rate differences between adults and adolescents for the following abbreviated item, which is a member of scales Pt and Sc:
“Have strange thoughts.”
(Endorsed true by 15% of MMPI-2 adult males and 10% of adult females, vs. 45% of boys in the MMPI-A normative sample and 46% of MMPI-A teenage girls.)
and to the following abbreviated item, a member of scales Pd, Pa, and Sc:
“Am misunderstood.”
(Endorsed true by 9% of adult men and 9% of adult women in the MMPI-2 normative sample, vs. 25.6% of adolescent boys and 37.4% of adolescent girls in the MMPI-A normative sample.)
and to the following abbreviated item, a member of the Mf and Si scales:
“Don’t mind not being better looking.”
(Endorsed true by 77% and 59% of the MMPI-2 male and female normative samples, respectively, vs. 49% of adolescent boys and 38% of adolescent girls in the MMPI-A normative sample.)
Psychological Development
Finally, a host of psychological and emotional tasks, including the processes of individuation, the formation of ego identity, and ego maturation, are accomplished during adolescence. Blos (1967) discussed individuation as a process involved with the development of relative independence from family relationships, the weakening of infantile object ties, and an increased capacity to assume a functional role as a member of adult society. Blos defined and described this task as similar to the more primitive struggle for individuation in the attainment of object constancy that occurs toward the end of the third year of life. Thus, the early adolescent has marked ambivalence concerning issues of independence versus dependence, particularly in terms of their relationships to their parents. This ambivalence is likely to be seen in rapid and marked attitudinal and behavioral changes by the adolescent (e.g., one moment protesting any parental involvement or supervision and the next moment regressing to marked dependency on mother or father).
Erikson (1956) described ego identity formation during adolescence as the assembly of converging identity elements that occur at the end of childhood, achieved through a process of normative crises. Ego identity was viewed by Erikson as including the conscious sense of individual identity as well as an unconscious striving for a continuity of personal character. In this process of ego formation, the ego integrates previous childhood identifications into a new totality, which lays the foundation of the adult personality. Positive resolution of this issue leads to a sense of ego identity, or continuity in one’s self-definition. Negative resolution of this challenge could result in ego diffusion, or uncertainty about who one is and what one will become in the future. This failure to achieve ego identity was related to the diagnostic category of identity problem (313.82) as described in the American Psychiatric Association’s (1994) Diagnostic and statistical manual of mental disorders (DSM-IV). Marcia (1966) further defined Erikson’s concept of ego identity in terms of two variables: commitment (whether or not the individual has accepted a set of values) and crisis (whether or not the individual has experienced an inner struggle in arriving at personal acceptance of a set of values). These two variables combine to yield four identity statuses in Marcia’s model: diffusion (no commitment, no crisis); foreclosure (commitment without crisis); moratorium (crisis without commitment); and achievement (commitment after crisis). Marcia argued that these categories, in the order given, represent developmental levels of increasingly advanced maturation.
The process of individuation is most clearly noted during early phases of adolescence, whereas the process of identity formation and consolidation is typically manifested during later stages of adolescence. As a result of these processes, adolescents will typically modify the way in which they interact and relate to others. Specifically, adolescents begin to increase their involvement with peers, while decreasing their immediate identification with family members. Further, the early stages of individuation may result in an increase in conflict with parents, as the adolescent ...