From the beginning, immunologists have maintained a unique nomenclature that has often mystified and even baffled their colleagues in other fields, causing them to liken immunology to a black box. With more than 1200 illustrations, the Illustrated Dictionary of Immunology, Third Edition provides immunologists and nonimmunologists a single-volume resource for the many terms encountered in contemporary immunological literature.
Encyclopedic in scope and including more than 1200 illustrations, the content ranges from photographs of historical figures to molecular structures of recently characterized cytokines, the major histocompatibility complex molecules, immunoglobulins, and molecules of related interest to immunologists. These descriptive illustrations provide a concise and thorough understanding of the subject.
To reflect modern advances, the third edition includes entries on immunopharmacology, newly described interleukins, comparative immunology, immunity to infectious diseases, and expanded definitions in all of the immunological subspecialities. Providing unprecedented breadth and detail, this readily accessible book is not only a pictorial reference but also a primary resource.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
Simplemente, dirígete a la sección ajustes de la cuenta y haz clic en «Cancelar suscripción». Así de sencillo. Después de cancelar tu suscripción, esta permanecerá activa el tiempo restante que hayas pagado. Obtén más información aquí.
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Illustrated Dictionary of Immunology un PDF/ePUB en línea?
Sí, puedes acceder a Illustrated Dictionary of Immunology de Julius M. Cruse, Robert E. Lewis en formato PDF o ePUB, así como a otros libros populares de Medizin y Immunologie. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
A rabbit immunoglobulin λ light chain allotype 100 designated as c7 and c21.
C domain
Refer to constant domain.
C gene
DNA encoding the constant region of immunoglobulin heavy and light polypeptide chains. The heavy chain C gene is comprised of exons that encode the different homology regions of the heavy chain.
C gene segment
DNA coding for a T cell receptor or an immunoglobulin polypeptide chain constant region. One or more exons may be involved. Constant region gene segments comprise immunoglobulin and T cell receptor gene loci DNA sequences that encode TCR α and β chains and nonvariable regions of immunoglobulin heavy and light polypeptide chains.
C region
Refer to constant region.
C region (constant region)
Abbreviation for the constant region carboxyl terminal portion of immunoglobulin heavy or light polypeptide chain that is identical in a particular class or subclass of immunoglobulin molecules. CH designates the constant region of the heavy chain of immunoglobulin, and CL designates the constant region of the light chain.
C segment
An exon that encodes an immunoglobulin molecule’s constant region domain.
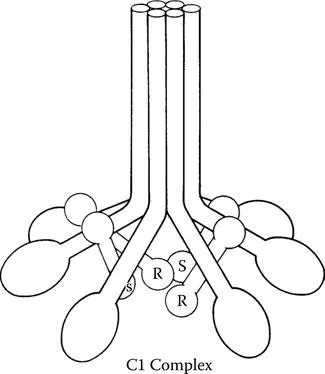
C1 Complex.
C1
A 750-kDa multimeric molecule comprised of one C1q, two C1r, and two C1s subcomponents. The classical pathway of complement activation begins with the binding of C1q to immunoglobulin M (IgM) or IgG molecules. C1q, C1r, and C1s form a macromolecular complex in a Ca2+-dependent manner. The 400-kDa C1q molecule possesses three separate polypeptide chains that unite into a heterotrimeric structure resembling a stem that contains an amino terminal in triple helix and a globular structure at the carboxyl terminus resembling a tulip. Six of these tulip-like structures with globular heads and stems form a circular and symmetric molecular complex in the C1q molecule that has a central core. The serine esterase molecules designated and C1s are needed for the complement cascade to progress. These single chain 85-kDa proteins unite in the presence of calcium to produce a tetramer comprised of two C1r and two C1s subcomponents to form a structure that is flexible and has a C1s–C1r–C1r–C1s sequence. When at least two C1q globular regions bind to IgM or IgG molecules, the in a tetramer associated with the C1q molecule becomes activated, leading to splitting of the C1r molecules in the tetramer with the formation of 57- and a 28-kDa chains. The latter, termed C1r, functions as a serine esterase, splitting the molecules into 57- and 28-kDa chains. The 28-kDa chain derived from the cleavage of C1s molecules, designated C1s, also functions as a serine esterase, cleaving C4 and C2 and causing progression of the classical complement pathway cascade.
C1 deficiencies
Only a few cases of C1q, C1r, or C1r and C1s deficiencies have been reported. The deficiencies have an autosomal-recessive mode of inheritance. Patients with these defects may manifest systemic lupus erythematosus (SLE), glomerulonephritis, or pyogenic infections. They exhibit increased incidence of type III (immune complex) hypersensitivity diseases. Half of C1q-deficient persons may contain physiologic levels of mutant C1q that are not functional.
C1 esterase inhibitor
A serum protein that counteracts activated C1. This diminishes the generation of C2b which facilitates development of edema.
C1 inhibitor (C1 INH)
A 478-amino acid residue, single polypeptide chain protein in the serum. It blocks C1r activation, prevents cleavage of , and inhibits C1s splitting of C4 and C2. The molecule is highly glycosylated, with carbohydrates making up approximately one half of its content. It contains seven O-linked oligosaccharides linked to serine and six N-linked oligosaccharides tethered to an asparagine residue. Besides its effects on the complement system, C1 INH blocks factors in the blood clotting system, including kallikrein, plasmin, factor XIa, and factor XIIa. C1 INH is an α2 globulin and is a normal serum constituent that inhibits serine protease. The 104-kDa C1 INH interacts with activated C1r or C1s to produce a stable complex that prevents these serine protease molecules from splitting their usual substrates. Either or can split C1 INH to uncover an active site in the inhibitor that becomes bound to the proteases through a covalent ester bond. By binding to most of the C1 in the blood, C1 INH blocks the spontaneous activation of C1. C1 INH binding blocks conformational alterations that would lead to spontaneous activation of C1. When an antigen–antibody complex binds C1, the inhibitory influence of C1 INH on C1 is relinquished. Genes on chromosome 11 in humans encode C1 INH. C1r and C1s subcomponents disengage from C1q following their interaction with C1 INH. In hereditary angioneurotic edema, C1 INH formation is defective. In acquired C1 INH deficiency, catabolism of C1 INH is elevated.
C1 inhibitor (C1 INH) deficiency
The absence of C1 INH is the most frequently found deficiency of the classic complement pathway and may be seen in patients with hereditary angioneurotic edema. This syndrome may be expressed as either a lack of the inhibitor substance or a functionally inactive C1 INH. The patient develops edema of the face; of the respiratory tract, including the glottis and bronchi; and of the extremities. Severe abdominal pain may occur with intestinal involvement. Because C1 INH can block Hagemann factor (factor XII) in the blood clotting mechanism, its absence can lead to the liberation of kinin and fibrinolysis resulting from the activation of plasmin. The disease is inherited as an autosomal-dominant trait. When edema of the larynx occurs, the patient may die of asphyxiation. When abdominal attacks occur, watery diarrhea and vomiting may occur. These bouts usually span 48 hours and are followed by a rapid recovery. During an attack of angioedema, C1r is activated to produce , which depletes its substrates C4 and C2. The action of activated C1s on C4 and C2 leads to the production of a substance that increases vascular permeability, especially that of postcapillary venules. C1 and C4 cooperate with plasmin to split this active peptide from C2. Of the families of patients with hereditary angioneurotic edema, 85% do not have C1 INH. Treatment is by preventive maintenance. Patients are given inhibitors of plasmin such as ε-aminocaproic acid and tranexamic acid. Methyl testosterone, which causes synthesis of normal C1 INH in angioneurotic edema patients, is effective by an unknown mechanism.
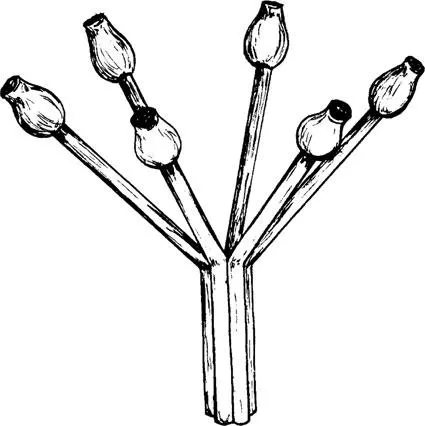
C1q
An 18-polypeptide-chain subcomponent of C1, the first component of complement. It commences the classical complement pathway. The three types of polypeptide chains are designated A, B, and C. Disulfide bonds link these chains. The triple helix structures of the C1q molecule are parallel and resemble the stems of six tulips in the amino terminal half of the structure. They then separate into six globular regions that resemble the heads of a tulip. The molecule is arranged in a heterotrimeric rod-like configuration, bearing a collagen-like triple helix at its amino terminus and a tulip-like globular region at its carboxyl terminus. The combination of six of the rod-shaped structures leads to a symmetric molecular arrangement comprised of three helices at one terminus and the globular (tulip-like) heads at the other terminus. The binding of antibody to C1q initiates the classic complement pathway. It is the globular C-terminal region of the molecule that binds to either immunoglobulin M (IgM) or IgG molecules. A tetramer comprised of two molecules of C1r and two molecules of C1s bind by Ca2+ to the collagen-like part of the stem. The C1q A chain and C1q B chain are coded for by genes on chromosome 1p in humans. The interaction of C1q with antigen–antibody complexes represents the basis for assays for immune complexes in patients’ serum. IgM, IgG1, IgG2, and IgG3 bind C1q, whereas IgG4, IgE, IgA, and IgD do not.
Clq.
C1q autoantibodies
Autoantibodies are detectable in 14 to 52% of patients with systemic lupus erythematosus (SLE), in 100% of patients with hypocomplementemic urticarial vasculitis syndrome (HUVS), in patients with rheumatoid arthritis (RA) (5% of patients with uncomplicated RA and 77% of RA patients with Felty’s syndrome), in 73% of patients with membranoproliferative glomerulonephritis type I, in 45% of patients with membranoproliferative glomerulonephritis types II and III, in 94% of patients of mixed connective tissue disease, and in 42% of patients with polyarteritis nodosa. Lupus nephritis patients usually reveal the immunoglobulin G (IgG) isotype. Rising levels of C1q autoantibodies portend renal flares in patients with SLE. The rare HUVS condition ca...