
eBook - ePub
Surgical Techniques in Total Knee Arthroplasty and Alternative Procedures
Saverio Affatato
This is a test
Compartir libro
- 298 páginas
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Surgical Techniques in Total Knee Arthroplasty and Alternative Procedures
Saverio Affatato
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Total knee arthroplasty (TKA) is commonly considered to be a reliable procedure, with high implant survival rates at 10 to 15 years of follow-up. The goal of total knee replacement surgery is to relieve pain and obtain better knee function. This is achieved by ensuring correct patient selection, pre-operative deformity, implant design and accurate surgical techniques. This book covers a range of techniques for the realisation of functional joint motion and stability. The first part of the book will describe fundamentals in total knee arthroplasty and alternative procedures. The second half will look at surgical techniques and considerations whilst the final chapters will address future trends and challenges in the field of knee surgery. This book will be an essential reference for academics, orthopaedic surgeons, and those training in medicine, physiatry and rheumatology.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Surgical Techniques in Total Knee Arthroplasty and Alternative Procedures un PDF/ePUB en línea?
Sí, puedes acceder a Surgical Techniques in Total Knee Arthroplasty and Alternative Procedures de Saverio Affatato en formato PDF o ePUB, así como a otros libros populares de Scienze biologiche y Biologia. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Información
Categoría
Scienze biologicheCategoría
BiologiaPart One
Fundamentals in total knee arthroplasty and alternative procedures
1
The history of total knee arthroplasty (TKA)
S. Affatato Istituto Ortopedico Rizzoli, Bologna, Italy
Abstract
The knee is a diarthrosis joint composed of four bones: the femur, the tibia, the patella, the proximal part of the fibula. Articular conformity between the femur and the tibia is provided by two fibrocartilagineous discs: the external and internal menisci. The knee ligaments are the anterior and posterior cruciate ligament, the internal and external collateral ligaments, and the patellar tendon.
Current total knee arthroplasty is made up of a femoral component and a tibial component of cobalt–chromium alloys, and a platform/insert of polyethylene.
Recently, oxidized zirconium or ceramic femoral components were used in the development of new TKAs.
Keywords
Knee anatomy
Femur
Tibia
Insert
Prostheses
1.1 Knee anatomy
Due to its anatomical complexity, the knee joint has not been definitively classified. It is widely categorized as a ginglymus (hinge joint). However, another approach is to regard it as two different joints: the tibio-femoral joint and the patello-femoral joint (Fig. 1.1). The tibio-femoral joint can be further sub-divided into two condyle joints between each femoral and tibial condyle.
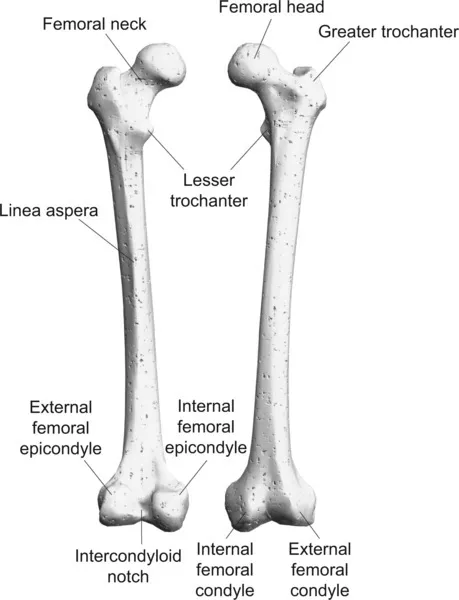
Figure 1.1 The tibio-femoral joint and the patello-femoral joint.
The patella can be found in front of the knee joint, a flat bone surrounded by the quadriceps tendon. The distal part of this tendon, called the patellar tendon, inserts into the tibial tuberosity connecting the patella with the tibia. The patello-femoral joint, an arthrodial (gliding) joint, allows the articular patella to glide over the patellar groove of the distal femur.
Therefore, in essence, the knee joint is a unique joint with three distinct components:
• the patello-femoral,
• the internal, and
• the external tibio-femoral compartments.
Enclosing the knee is the articular capsule, a fibrous membrane connecting the bones to each other.
Synovial fluid produced in the synovial membrane provides lubrication for the joint and supply of nutrient for the articular cartilage. The synovial membrane can be found on the internal surface of the articular capsule coating the articular cavity and, in particular, in the deep recess beneath the quadriceps tendon. The presence of ligaments and tendons ensures the stability of the joint. The most important ligaments of the knee are the anterior and posterior cruciate ligaments, the internal and external collateral ligaments and the patellar tendon.
The external and internal menisci are two fibrocartilaginous discs above each tibial condyle, which improve congruity between the femur and the tibia. They cover the outer part of the tibial articular facets. The menisci look like a wedge, being thicker toward the periphery of the tibial condyles. While the external meniscus is approximately circular, the internal meniscus has a semicircular shape. The external and internal menisci are connected anteriorly by the transverse ligament. The coronary ligaments, which are part of the articular capsule, connect the menisci with the tibia along its peripheral portion. The menisci cushion the compressive force and increase the stability of the knee, particularly the internal meniscus since it is tightly anchored to the bone (Gray 1918; Kapandji, 1998) (Fig. 1.2).
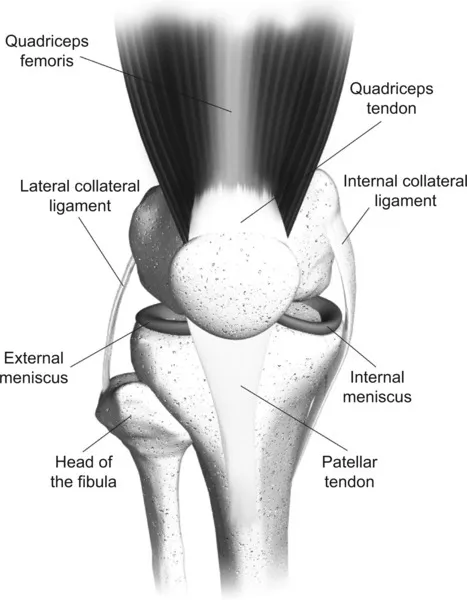
Figure 1.2 Representation of menisci anchored to the bone.
1.2 History of total knee arthroplasty (TKA)
The first attempt at treating patients affected by knee osteoarthritis was during the mid nineteenth century. This consisted of interposing a soft tissue between the joint surfaces or removing a portion of bone from both the distal femur and proximal tibia.
In 1880 the German surgeon Theophilus Gluck fixed ivory prosthetic components to the bone by means of plaster (Gluck, 1890); this can be regarded as the earliest example of total joint replacement. After that, no notable progress was made until 1973, when the prototype of the modern knee prostheses was proposed by John Insall and his colleagues (Insall et al., 1974). This prototype comprised a metallic femoral component and plastic tibial and patellar components, all fixed to the bone. The geometry of the prosthetic components ensured joint stability even if the cruciate ligaments were both sacrificed. All the components were fixed to the bone with cement, made of colophony, pumice and plaster of Paris.
Further progress occurred over the next few years, leading to the use of a metal back for the tibial component and posterior cruciate ligament retention. In the early twentieth century, interposition arthroplasty using autologous tissue or metallic components came to the fore and in 1950s the first tibia replacement was carried out by McKeever (McKeever, 1960). From then, the vision of knee arthroplasty took two different routes:
• the constrained (or hinged) prosthesis, and
• the condylar replacement.
In the condylar replacement knee prosthesis the distal femoral and proximal tibial bearing surfaces are substituted with unconnected artificial components with no direct mechanical link between them. The original design named the Freeman-Swanson prosthesis and proposed at the end of the 1960s at Imperial College, London, comprised a metal “roller” placed on the distal femur articulating with a polyethylene tibial tray. This first prototype required a re-section of both cruciate ligaments. Later, uni-compartmental knee arthroplasty was developed, involving the substitution of only one tibio-femoral compartment, with the aim of preserving part of the bone. Recent improvements have introduced newer bearings options and cementless fixing (Ranawat). The surgical performance and clinical outcome of knee replacement surgery is constantly being improved by computer-aided systems which assist the surgeon in accurately positioning the prosthesis. Due to its excellent long-term clinical results, knee replacement is a successful and promising procedure. Consequently, the rate of total knee replacement is expected to increase in the future (Culliford et al., 2010).
The aim of TKA is the re-establishment of joint function and the alleviation of pain. The main cause of joint impairment is primary osteoarthritis, a degenerative condition due to ageing. Another condition necessitating TKA is secondary osteoarthritis as a result of an altered load distribution around the knee, generally due to post-traumatic disorders (fractures of the distal femur or proximal tibia) or congenital anomalies producing varus or valgus alignments. Other indications for TKA include osteonecrosis of the femoral condyles (Radke et al., 2005), rheumatoid arthritis (Meding et al., 2004) and haemophilic arthropathy (Goddard et al., 2010).
1.3 Indications for a TKA
TKA is indicated when the knee joint is severely damaged by osteoarthritis, rheumatoid arthritis or other diseases. The primary purpose of TKA is to restore joint stability and relieve pain caused by severe arthritis. The pain should be significant and disabling. Loss of joint stability and chronic acute pain result in a significant reduction in the quality of life. Correction of significant deformity is another important indication but is rarely used as the primary reason for surgery. Generally, TKA is appropriate for older patients with more modest activities, as the TKA lifetime is finite and is adversely affected by higher activity levels (Ranawat et al., 1993; Ritter et al., 1994), (Canale ST and Beat...