
eBook - ePub
Evidence-Based Physical Therapy for the Pelvic Floor
Bridging Science and Clinical Practice
Kari Bo, Bary Berghmans, Siv Morkved, Marijke Van Kampen
This is a test
Compartir libro
- 448 páginas
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Evidence-Based Physical Therapy for the Pelvic Floor
Bridging Science and Clinical Practice
Kari Bo, Bary Berghmans, Siv Morkved, Marijke Van Kampen
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Bridging the gap between evidence-based research and clinical practice, Physical Therapy for the Pelvic Floor has become an invaluable resource to practitioners treating patients with disorders of the pelvic floor. The second edition is now presented in a full colour, hardback format, encompassing the wealth of new research in this area which has emerged in recent years.
Kari Bø and her team focus on the evidence, from basic studies (theories or rationales for treatment) and RCTs (appraisal of effectiveness) to the implications of these for clinical practice, while also covering pelvic floor dysfunction in specific groups, including men, children, elite athletes, the elderly, pregnant women and those with neurological diseases. Crucially, recommendations on how to start, continue and progress treatment are also given with detailed treatment strategies around pelvic floor muscle training, biofeedback and electrical stimulation.
- aligns scientific research with clinical practice
- detailed treatment strategies
- innovative practice guidelines supported by a sound evidence base
- colour illustrations of pelvic floor anatomy and related neuroanatomy/ neurophysiology
- MRIs and ultrasounds showing normal and dysfunctional pelvic floor
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Evidence-Based Physical Therapy for the Pelvic Floor un PDF/ePUB en línea?
Sí, puedes acceder a Evidence-Based Physical Therapy for the Pelvic Floor de Kari Bo, Bary Berghmans, Siv Morkved, Marijke Van Kampen en formato PDF o ePUB, así como a otros libros populares de Medicine y Physiotherapy, Physical Medicine & Rehabilitation. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Información
Chapter 1
Overview of physical therapy for pelvic floor dysfunction
Kari Bø
Pelvic floor dysfunction
The framework of this book is based on the approach to disorders of the pelvic floor in women described by Wall and DeLancey (1991). Wall and DeLancey (1991) stated that ‘pelvic floor dysfunction, particularly as manifested by genital prolapse and urinary or faecal incontinence, remains one of the largest unaddressed issues in women’s health care today’ (p. 486). In their opinion, lack of success in treating patients with pelvic floor dysfunction is due to a professional ‘compartmentalization’ of the pelvic floor.
Each of the three outlets in the pelvis has had its own medical specialty, with the urethra and bladder belonging to the urologist, the vagina and female genital organs belonging to the gynaecologist, and the colon and rectum belonging to the gastroenterologist and the colorectal surgeon (Fig. 1.1).
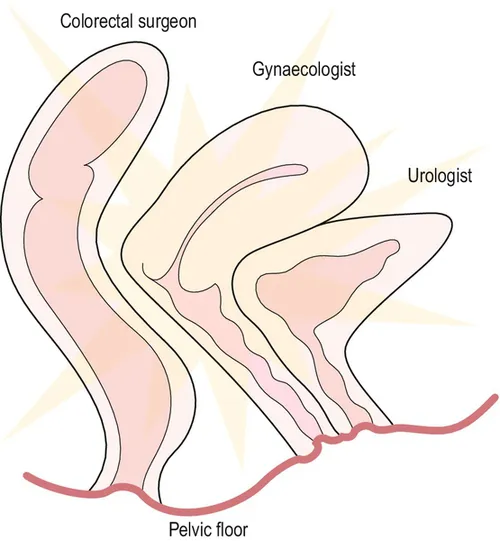
Figure 1.1 Gynaecologists, urologists and colorectal surgeons concentrate on their areas of interest and tend to ignore the pelvic floor common to them all.
Wall and DeLancey (1991) argue that instead of concentrating on the three ‘holes’ in the pelvis, one should look at the ‘whole pelvis’, with the pelvic floor muscles (PFM), ligaments and fasciae as the common supportive system for all the pelvic viscera.
The interaction between the PFM and the supportive ligaments was later elaborated by DeLancey (1993) and Norton (1993) as the ‘boat in dry dock theory’. The ship is analogous to the pelvic organs, the ropes to the ligaments and fasciae and the water to the supportive layer of the PFM (Fig. 1.2). DeLancey (1993) argues that as long as the PFM or levator ani muscles function normally, the pelvic floor is supportive and the ligaments and fascia are under normal tension. When the PFM relax or are damaged, the pelvic organs must be held in place by the ligaments and fasciae alone. If the PFM cannot actively support the organs, over time the connective tissue will become stretched and damaged.
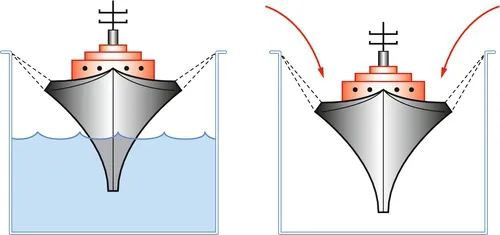
Figure 1.2 The ‘boat in dry dock’ analogy. Reproduced with permission from Norton, 1993.
Bump and Norton (1998) also used this theoretical framework in their overview of the epidemiology and natural history of pelvic floor dysfunction. They suggested that pelvic floor dysfunction may lead to the following conditions:
• urinary incontinence (stress, urge and mixed incontinence);
• faecal incontinence;
• pelvic organ prolapse;
• sensory and emptying abnormalities of the lower urinary tract;
• defecatory dysfunction;
• sexual dysfunction;
• chronic pain syndromes.
Bump and Norton (1998) also described three stages in the development of pelvic floor dysfunction:
1. A perfect pelvic floor that is anatomically, neurologically and functionally normal.
2. A less than perfect, but well-compensated pelvic floor in an asymptomatic patient.
3. A functionally decompensated pelvic floor in the patient with end-stage disease, with urinary incontinence, anal incontinence, or pelvic organ prolapse.
A model describing aetiological factors possibly leading to or causing pelvic floor dysfunction in women has been developed, classifying the factors into:
• predisposing factors (e.g. gender, genetic, neurological, anatomical, collagen, muscular, cultural and environmental);
• inciting factors (e.g. childbirth, nerve damage, muscle damage, radiation, tissue disruption, radical surgery);
• promoting factors (e.g. constipation, occupation, recreation, obesity, surgery, lung disease, smoking, menstrual cycle, infection, medication, menopause);
• decompensating factors (e.g. ageing, dementia, debility, disease, environment, medications).
In 2008 DeLancey et al further developed this model to what they named the Lifespan Model. They described a graphical tool to integrate pelvic floor function related to pelvic floor disorders in three major phases: (1) development of functional reserve during an individual’s growth; (2) variations in the amount of injury and potential recovery that occur during and after vaginal birth; and (3) deterioration occurring with advancing age. The authors suggest that the Lifespan Model should be used to focus on more refined preventive strategies of pelvic floor dysfunction risk in an individual woman as opposed to more general recommendations for all women (DeLancey et al., 2008).
Wall and DeLancey (1991) argued that progress in the treatment of pelvic floor dysfunction in women would occur more rapidly if a unified, cross-disciplinary approach to disorders of the pelvic support was developed. Wall and DeLancey (1991) mentioned only the different medical professions as part of a multidisciplinary team. In this book we will argue that physical therapists (PTs), having assessment and treatment of the musculoskeletal system in general as their specialty, should be core professionals in a multidisciplinary approach to pelvic floor dysfunction.
Physical therapy for the pelvic floor
The nature of physical therapy
In May 1999, at the 14th General Meeting of the World Confederation for Physical Therapy (WCPT), a position statement describing the nature and process of physical therapy/physiotherapy was approved by all member nations (WCPT, 1999). This description will be used as a foundation and framework to give an overview of physical therapy/physiotherapy in the area of pelvic floor dysfunction. The term ‘physical therapy’ will be used throughout this book, in accordance with the guidelines of the WCPT Europe.
According to the WCPT, physical therapy is ‘providing services to people and populations to develop, maintain and restore maximum movements and functional ability throughout the lifespan’. The main area of practice for PTs is musculoskeletal pain and dysfunction. However, many PTs also specialize in other areas, such as the cardiorespiratory field, neurology and coronary disease. In all areas, PTs aim to improve functional capacity and improve patients’ ability to maintain or increase physical activity level.
The PFM are not responsible for gross motor movements alone, but work in synergy with other trunk muscles. Therefore, pelvic floor dysfunction may lead to symptoms during movement and perceived restriction in the ability to stay physically active (Bø et al., 1989; Nygaard et al., 1990). Several studies have shown that, for example, urinary incontinence may lead to a change in movement patterns during physical activities (Bø et al., 1989; Nygaard et al., 1990), withdrawal from regular fitness activities and troublesome difficulties when being active (Brown and Miller, 2001; Nygaard et al., 1990).
Lifelong participation in regular moderate physical activity is important in the prevention of several diseases, and is an independent factor in the prevention of osteoporosis, obesity, diabetes mellitus, high blood pressure, coronary heart disease, breast and colon cancer, depression and anxiety (Bouchard et al., 1993).
In addition, limitations in the ability to move or conduct activities of daily living either due to age or injuries, may also lead to other problems, such as secondary incontinence. Physical therapy for pelvic floor dysfunction may therefore also include physical activities for increasing general function and fitness level.
Physical therapy includes the provision of services in circumstances where movement and function are threatened by the process of ageing or that of injury or disease.
WCPT
Hippocrates (5th to 4th centuries bc) claimed that ‘all parts of the body which have a function, if used in moderation and exercised in labours in which each is accustomed, become thereby healthy, well-developed and age more slowly, but if unused and left idle they become liable to disease, defective in growth, and age quickly’.
The PFM are subject to continuous strain throughout the lifespan. In particular, the pelvic floor of women is subject to tremendous strain during pregnancy and childbirth (Mørkved, 2003; DeLancey et al., 2008). In addition, hormonal changes may influence the pelvic floor and pelvic organs and a decline in muscle strength may occur due to ageing. Hence, the PFM may need regular training to stay healthy throughout life.
Physical therapy is concerned with identifying and maximizing movement potential, withi...