
eBook - ePub
Current Therapy in Equine Reproduction
Juan C. Samper, Angus O. McKinnon, Jonathan Pycock
This is a test
Compartir libro
- 512 páginas
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Current Therapy in Equine Reproduction
Juan C. Samper, Angus O. McKinnon, Jonathan Pycock
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Offering the most current insights on horse breeding, this book covers the entire reproductive system, normal and abnormal mare physiology, and a wide range of reproductive problems commonly seen in both the mare and stallion. Coverage includes advanced reproductive techniques, with numerous breeding strategies to help you achieve optimal fertility rates.
- Features the most current information available on equine reproduction, including the latest therapies and treatments for breeding dysfunction, as well as advances in reproductive techniques
- Focuses on therapy and treatment to provide practitioners with quick access to key information
- Features the shared experience and valuable advice of world-renowned experts who have first-hand knowledge of which treatments and therapies are most effective
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Current Therapy in Equine Reproduction un PDF/ePUB en línea?
Sí, puedes acceder a Current Therapy in Equine Reproduction de Juan C. Samper, Angus O. McKinnon, Jonathan Pycock en formato PDF o ePUB, así como a otros libros populares de Medicina y Scienza veterinaria equina. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Información
Categoría
MedicinaCategoría
Scienza veterinaria equinaSECTION VII
THE PREGNANT MARE: DIAGNOSIS AND MANAGEMENT
CHAPTER 52Pregnancy Diagnosis in the Mare*
FERTILIZATION
The uterine tube has the ability to transport sperm toward the ovary while transporting the ovum in the opposite direction. Fertilization of the ovum occurs in the oviduct in mares. The fertilized egg or conceptus then takes 5 to 6 days to reach the uterus.
EMBRYONIC AND FETAL DEVELOPMENT
The conceptus is highly mobile throughout the entire uterus until day 16 after ovulation. The early movement of the conceptus is thought to play a key role in the physiologic event known as maternal recognition of pregnancy. The mobility phase ends when the conceptus becomes stationary and “fixation” occurs at the base of the right or left uterine horn. Fixation in postpartum mares tends to occur in the previously nongravid horn. Implantation occurs gradually and relatively late in the mare, beginning around day 40. It is not complete until approximately day 140. By convention, the term embryo is used up to day 40 and the term fetus after day 40.
Endometrial cups are a unique feature of the equine placenta. On or about day 28 of gestation, the chorionic girdle begins to form at the junction of the yolk sac and allantoic membranes. Specialized cells from the chorionic girdle invade the underlying uterine epithelium between days 36 and 38. Once in the endometrium, they enlarge and become clumped together to form the endometrial cups. The cups are arranged in a circle at the base of the gravid uterine horn. Endometrial cups produce equine chorionic gonadotropin (eCG), which stimulates the primary corpus luteum (CL) and causes induced secondary follicles to ovulate and/or luteinize. Because progesterone production remains high, mares do not show signs of estrus at the time of these secondary ovulations. This is independent from the presence of a fetus, so once the endometrial cups are formed, eCG production will proceed even in instances in which embryonic or fetal loss occurs.
ROUTINE PREGNANCY DIAGNOSIS
It is important to be able to tell if a mare is pregnant for management and husbandry reasons: Pregnant mares should be managed differently from nonpregnant mares. They should have further examinations to monitor the development of the pregnancy, confirm the absence of twin pregnancies, and monitor for early embryonic or fetal death. Twin pregnancies are bad news in the mare, and if the pregnancy is diagnosed early enough, appropriate intervention is possible (see Chapter 54).
It is just as important to identify the nonpregnant mare as soon as possible. Some mares have prolonged luteal activity (previously termed “persistent corpus luteum”), and the maintenance of circulating progesterone concentrations in these nonpregnant mares means that they do not spontaneously return to estrus. Persistence of luteal activity in the nonpregnant mare is a major cause of subfertility and is the main cause of anestrus during the breeding season. Traditionally, the term “prolonged diestrus” has been used to describe a condition in which the function of the CL continues beyond its normal cyclic lifespan of 15 to 16 days, resulting in the maintenance of elevated circulating progesterone concentrations for longer than expected. The term prolonged luteal activity is preferred, because “persistent diestrus” implies that the CL persists, whereas it is possible that other CLs are formed sequentially from diestrous ovulations. Prolonged luteal activity occurs in up to 20% of estrous cycles and are not accompanied by estrus; the cervix will remain pale in color, dry, and tightly closed. If diestrous ovulations occur late in the luteal phase, they will be refractory to the effect of endogenous luteolysins, resulting in a persistent luteal phase. Such abnormal luteal activity is associated with significant problems in reproductive management because affected mares may erroneously be assumed to be pregnant.
Plasma progesterone profiles are indistinguishable from those of pregnant animals. The uterus becomes firm and tubular (tonic) and the cervix is typical of that of pregnancy. Transrectal ultrasound imaging fails to detect a conceptus, but a CL can be detected in the ovary (Fig. 52-1, A and B). The ability to detect the CL throughout diestrus represents a profound diagnostic advantage of ultrasonography over rectal palpation.
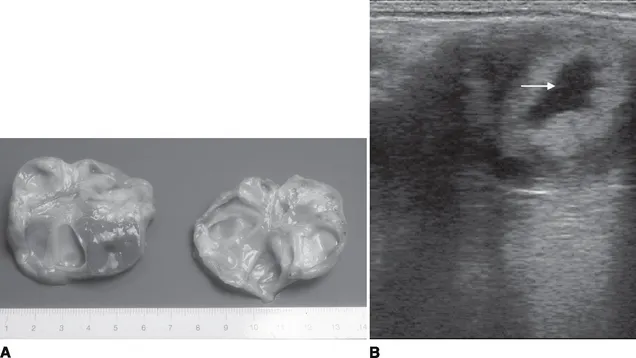
Figure 52-1A, Gross specimen of left and right ovaries cut in half, showing a corpus luteum visible in the left ovary. A small central space can be seen in the corpus luteum. B, An ultrasound image of the equine corpus luteum with a centrally located anechoic area (arrow). The equine corpus luteum may remain uniformly echoic throughout its period of detection, or as in this image, an anechoic area may develop. In fact, a continuous distribution from uniformly echoic through to almost completely anechoic can be appreciated, with only a small border of luteal tissue.
Failure of synthesis and/or release of prostaglandin F2α(PGF2α) at the end of diestrus and failure of the corpus luteum to respond to PGF2αare the most likely causes of persistence of the CL. Treatment is by injection of a luteolytic dose of PGF2αor a synthetic analogue. The interval between treatment and ovulation varies considerably depending on the size of follicles at the time of treatment. Therefore, ultrasonographic examination of the mare before such treatment is always advisable in order to assess the status of folliculogenesis.
A clinical examination by a veterinary surgeon involving rectal palpation and ultrasound evaluation of the internal organs is the most accurate and useful method of pregnancy diagnosis. Nonetheless, several potential pitfalls have been recognized, including the confusion of uterine cysts for conceptuses and the presence of multiple conceptuses.
Speculum Examination of the Cervix
The vagina and cervix of the early pregnant mare are covered in pale, dry mucous membranes. The cervix is closed and resembles exactly the cervix of the mare in diestrus. As the pregnancy progresses, the external opening of the cervix becomes covered in tacky, dry mucus. Later in pregnancy (after 6 months), the cervix can be very relaxed.
Rectal Examination
Cervix
In early pregnancy (16 to 30 days), the cervix can be palpated on the floor of the pelvis as a rigid, firm structure (as during diestrus).
Ovaries
Both ovaries should be palpated, although ovarian palpation contributes little to pregnancy diagnosis. This is because both ovaries usually are enlarged from 18 to 40 days as a result of follicular development and the CL is not palpable. From 40 to 120 days, extensive ovarian activity with ovulations, luteinization, and development of secondary corpora lutea is evident. Follicular activity decreases from 120 days to term, and the ovaries become small and inactive. The position of the ovaries up to 60 days of pregnancy is as for the nonpregnant mare. From then on, they are drawn cranially and medially but remain dorsal to the uterus. From 5 months of pregnancy onward, the ovaries usually are not palpable.
Uterus
Both uterine horns and body should be palpated. Pregnancy diagnosis is based on tone and...