
eBook - ePub
Essential Geriatrics
Henry Woodford
This is a test
Compartir libro
- 492 páginas
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Essential Geriatrics
Henry Woodford
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
In an ageing society, developing high-quality healthcare for older people becomes increasingly important. This revised and updated fourth edition focuses on the key aspects of ageing and healthcare for older people, especially those with moderate to severe frailty. It has expanded sections on the key topics of frailty and medicines optimisation with evidence from critically appraised clinical trials formulated into practical guidance for management. It details the non-pharmacological management of cognitive disorders and models of person-centred care. Additional topics of acute coronary syndromes and COVID-19 have also been added in this comprehensive text for healthcare professionals.
Key Features
- Provides practical therapeutic advice including deprescribing decisions for all medication types.
-
- Presents statistics in more clinically meaningful ways – i.e. number needed to treat and no p-values, to aid the process of shared decision-making for clinicians and professionals.
-
- Includes 200 revised questions and answers throughout the text in the 'best of five' format suitable for the SCE and similar higher-training exams.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Essential Geriatrics un PDF/ePUB en línea?
Sí, puedes acceder a Essential Geriatrics de Henry Woodford en formato PDF o ePUB, así como a otros libros populares de Medicina y Geriatría. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Part B
Brain
6
Dementia
DOI: 10.1201/9781003240389-9
Definition
Dementia is a syndrome attributed to disease of the brain, usually of a chronic or progressive nature, in which there is a disturbance of multiple brain functions. These impairments may include calculation, learning capacity, language and judgement. It is usually only considered present when there is a resultant impact on social or occupational function. Consciousness is usually unaltered. There may also be deterioration in emotional control, social behaviour or motivation. In other words, it is not simply memory loss but a complex condition that affects multiple aspects of cognition.
We should not ‘suffer from’, but instead ‘live with’ dementia. People with cancer are not defined as cancerous, people with dementia should not be defined as demented.
Epidemiology
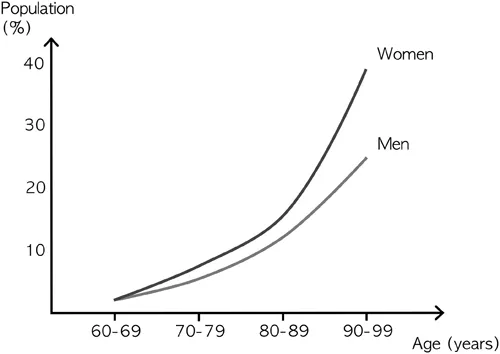
The prevalence of dementia rises from around 2% of people aged in their 60s to around 25% of men and 39% of women aged in their 90s (see Figure 6.1).1 These figures represent, roughly, a doubling in prevalence for every five-year increase in age. A more positive thought is that around two-thirds of the very old do not have dementia. However, prevalence is higher among hospitalised older people, being present in around half of those aged 80–89 and two-thirds of those aged over 90.2 Around a quarter of hospital beds overall and around 40% of acute medical beds are occupied by people with dementia (some previously undiagnosed).3, 4 This can skew the perception of old age for those who mainly see older people in healthcare settings. Around a third of people with dementia live in care homes.5
Although ageing of the population has resulted in an increased number of people with dementia, recent studies have suggested that the age-specific incidence of dementia has been falling over the last couple of decades (by 1 to 3% per year).6–8 This is probably related to improved lifestyle factors. In addition to dementia, there is a significant number of individuals who have some clinical evidence of cognitive impairment that is not severe enough to satisfy the diagnostic criteria for dementia (termed ‘mild cognitive impairment’ – see page 114). However, cognitive decline is not an inevitable feature of ageing and many older people continue to function at their baseline level (see page 11).9
Life expectancy is reduced in people with dementia. Estimates of average survival from the time of symptom onset are typically in the range of 3.3 to 11.7 years, and survival from diagnosis in the range of 3.2 to 6.6 years.10 Survival time is influenced by age and severity at the time of diagnosis. Studies suggest an average survival from diagnosis of 7–11 years for people aged 65–69, 4–5 years for those aged 70–79, 3–4 years for those aged 80–89 and 2–3 years for those over 90.11, 12 Life expectancy in advanced dementia is, on average, in the region of one year. These data can be compared to average data for the whole population (see page 6). Dementia is now the leading cause of death in people aged over 80 in the UK. In 2019 in England and Wales, the deaths of 15% of men and 23% of women aged over 80 were due to conditions related to dementia.13
Cognition
Attention
Attention is the ability to focus on a task and is determined by both concentration and arousal. It is mediated by the reticular activating system, which is a complex series of connections between the cerebral cortex, thalamus and the reticular formation (a ‘net-like’ collection of cells in the brainstem). In the presence of reduced attention, other brain functions are also impaired.
Memory
Traditionally, memory function has been loosely divided into short-term and long-term components. More recently, memory has been classified into four categories,14 these are outlined below:
- Episodic memory: The memory of specific personal events and experiences, for example, what you did on holiday last year. Predominantly mediated by the medial temporal lobes and limbic system (including the hippocampus – see Figure 6.7). Insults to this system tend to affect recently learned memories more than older ones (i.e. short-term memory is more affected than long-term memory).
- Semantic memory: Knowledge of the world not related to personal experiences. This includes the names of objects, for example, the names of animals. This is predominantly mediated by the inferolateral temporal lobes.
- Procedural memory: The memory of how to perform tasks, such as riding a bike. The basal ganglia and cerebellum predominantly mediate this. It occurs at a subconscious level. It may be particularly affected in movement disorders (see Chapter 9).
- Working memory: Short-term (seconds to minutes) ‘keeping it in your head’. It can be phonologic (e.g. a phone number) or spatial (e.g. manipulating an object in your mind). The prefrontal cortex is important in this process along with other brain areas depending on the nature of the task. For an effective working memory, it is also necessary to be able to maintain attention/concentration.
Memories may be conscious (declarative) or non-conscious (non-declarative). Confabulation is the making-up of new ‘memories’ to replace those that have been lost. Memory impairment is common to many disorders, including dementia, delirium and depression.
Language
The dominant hemisphere encodes language. This is the left side of the brain in all right-handed and most left-handed people. The language centres are more diffuse and less well defined than traditionally thought. They include Broca’s area in the frontal lobe and Wernicke’s area at the margin of the temporal and parietal lobes. There is also a network of connections between these areas, called the arcuate fasciculus (see Figure 6.2). Paraphrasia is a term for the use of abnormal or incorrect words. These can be semantic (similar categories – e.g. dog for cat), phonemic (similar sounds – e.g. jar for car) or neologistic (made up words – e.g. flut for car). Prosody is a term for the melodic characteristics of speech including intonation, stress and cadence (rhythm). Anomia is a term for a naming deficit (e.g. cannot say the name for a pen). Anomic aphasia is also called ‘word block’. With this disorder, people typically stop mid-sentence. Its presence is associated with space occupying lesions within the dominant lobe. Progressive aphasia is a term for a slowly worsening non-fluent aphasia secondary to left frontotemporal degeneration (plus apraxia). Dysgraphia (impaired writing) and dysle...