![]()
Background
1
Introduction
This Manual is written for psychiatrists, psychologists, primary care physicians, nurses, and all persons involved in treating patients with major depression (unipolar and bipolar) in a clinical or ambulatory setting. The aim is first, to present the theory behind these non-pharmaceutical chronobiological treatments; second, to document the evidence that they are efficacious in controlled trials, and third, to provide a handbook for step-by-step implementation of these therapies in everyday practice. The theoretical chapters can be skipped, and the interventions still be effectively applied. Selected references focus on new reviews and clinically relevant studies that will lead the reader to the original research.
1.1
Unmet Needs in the Treatment of Depression
Much progress has been made in dissecting the Anatomy of Melancholy since Robert Burton wrote his extensive treatise in 1621 (fig. 1). Those involved in treating patients with depression know that we have many evidence-based treatments, from psychotherapy to psychopharmacology. Important developments in the treatment of major depression over the last decades include cognitive behavioural therapy, SSRIs , and mixed NA/5HT reuptake inhibitors, both with a better side-effect profile than the classic tricyclics. Yet we have not attained our goal, the right treatment for every patient and the minimisation of residual symptoms. None of these treatments has broken the time barrier with fast onset of action, which remains the crux for clinicians who need to carefully monitor patients in the critical period until antidepressants begin to work. The slow action of antidepressants is particularly worrisome for severely depressed or suicidal patients. Furthermore, not all patients respond to all drugs, and it usually takes an odyssey through various medications and their combinations to find the right mix. And, although responding, many patients show residual symptoms – which increases the risk of relapse.
There is an intensive search for new psychopharmacologic agents. Antidepressants based on classic neurotransmitter systems are still a prime focus, but there are many novel drug targets other than monoamines. Strategies that promote adjuvant therapy are on the increase, whether a combination with other medications (e.g. pindolol, thyroid hormone) or psychological interventions (e.g. cognitive behavioural therapy).
We already have the means to speed up response without waiting for that miracle drug – or using the most powerful and rapid, yet unwieldy tool, electroconvulsive therapy (ECT). Chronobiological treatments are well tested and efficacious. They can be combined with any medication conventionally used for major depression. Light therapy has undergone widespread controlled, randomised clinical trials, particularly – but not only – in seasonal affective disorder (SAD). Light therapy is accepted worldwide as the treatment of choice for SAD ; recent research focus has moved to non-seasonal depression, where studies are now showing that adjuvant light induces faster and greater antidepressant response.
Sleep deprivation has been widely studied for more than four decades. Were sleep deprivation an easily-administered pill, it would be the treatment of choice for major depression, with an amazing onset of action within hours in approximately 60% of patients. The data documenting its efficacy – gathered mostly in Europe – are unambiguous, convincing and replicable. There are several reasons why this therapy has not been incorporated into everyday psychiatric practice. One is psychological: the patient who suffers insomnia is asked to remain without sleep – is this a joke, a torture, or ignorance of the miseries of the sleep disturbances intrinsic to depression? If one changed the name, would the attitude and acceptance change? Would we enthusiastically treat patients with ‘wake therapy’ even though we shy from attempting ‘sleep deprivation’?
Fig. 1. Frontispiece of Robert Burton’s The Anatomy of Melancholy, ed.7, 1660.
Combining these methods with medication has hardly been tried. There has been no consensus development and no lobby for widespread education and application. It may be because companies cannot patent these treatments – there is no profit motive. These non-pharmaceutical, biologically based therapies are not only powerful adjuvants, but also antidepressants in their own right. We have a responsibility to offer them to our patients. There are practically no side effects, they are cost-effective, and we expect that they will shorten the length of hospitalisation.
The International Society for Affective Disorders (ISAD) convened a Committee on Chronotherapeutics to review chronobiologic treatments for depression (https://www.isad.org.uk/committees/chrono_therapy.asp). The report was published as an editorial in Psychological Medicine [2]. The recommendations are summarised in table 1, the list of chronotherapeutic modalities in table 2.
This Manual provides theoretical and practical guidelines for implementing wake therapy and light treatment in clinical practice. It fulfils an objective of our non-profit organisation (Center for Environmental Therapeutics, www.cet.org) to provide research-based, reliable information about these non-pharmacologic treatments. While our focus is on hospitalised patients, light therapy is easily applied to outpatients, and wake therapy can be offered in ambulatory centres (section 7).
Table 1. Recommendations of the Committee on Chronotherapeutics of the International Society for Affective Disorders (ISAD) [2]
1 | Sleep deprivation (wake therapy) is the most rapid antidepressant available today: approximately 60% of patients, independent of diagnostic subtype, respond with marked improvement within hours. Treatment can be a single or repeated sleep deprivation, total (all night) or partial (second half of the night). Relapse can be prevented by daily light therapy, concomitant administration of SSRIs , lithium (for bipolar patients), or a short phase advance of sleep over 3 days following a single night of wake therapy. Combinations of these interventions show great promise. |
2 | Light therapy is effective for major depression – not only for the seasonal subtype. As an adjuvant to conventional antidepressants in unipolar patients, or lithium in bipolar patients, morning light hastens and potentiates the antidepressant response. Light therapy shows benefit even for patients with chronic depression of 2 years or more, outperforming their weak response to drugs. This method provides a viable alternative for patients who refuse, resist or cannot tolerate medication, or for whom drugs may be contraindicated, as in antepartum depression. |
3 | Given the urgent need for new strategies to treat patients with residual depressive symptoms, clinical trials of wake therapy and/or adjuvant light therapy, coupled with follow-up studies of long-term recurrence, are a high priority. |
Table 2. Circadian and wake therapies for major depression
| Therapeutic response |
| latency | duration |
| Total sleep deprivation = wake therapy (WT) | hours | ~1 day |
| Partial sleep deprivation 2nd half of the night (PWT) | hours | ~1 day |
| Repeated WT or PWT | hours | days/weeks |
| Repeated WT or PWT with antidepressants | hours | weeks/months |
| Phase advance of the sleep-wake cycle | ~3 days | 1-2 weeks |
| WT followed by sleep phase advance | hours | 1-3 weeks |
| Single/repeated WT or PWT + light therapy | hours | weeks |
| Single/repeated WT or PWT + phase advance + light therapy | hours | weeks |
| Single/repeated WT or PWT + lithium, pindolol, or SSRIs | hours | months |
| Light therapy (winter seasonal depression) | days | weeks/months |
| Light therapy (nonseasonal depression) | weeks | weeks/months |
| Light therapy + SSRIs (nonseasonal depression) | 1-2 weeks | weeks/months |
| Dark or rest therapy for mania or rapid cycling | days | throughout maintenance of treatment |
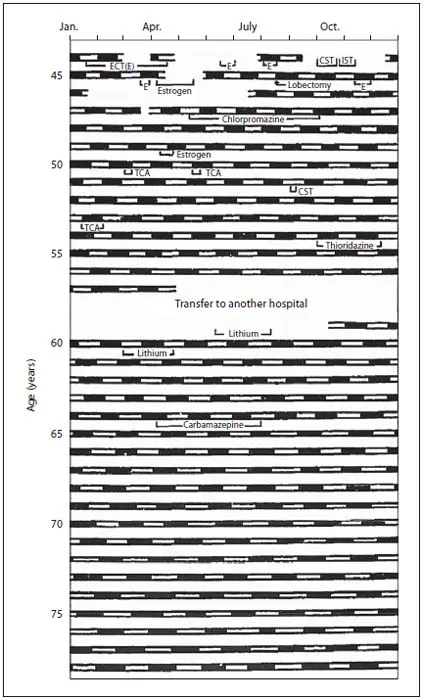
Fig. 2. Clinical record (35 years) of a rapid-cycling bipolar woman with 2- to 4-day cycles of depression (black bars) and mania (white bars). No drug treatment affected the periodicity. CST = Continuous sleep therapy; IST = insulin shock therapy; TCA = tricyclic antidepressant. From Mizukawa et al. [3], with permission.
1.2
Role of Biological Rhythms in Psychiatry
One of the most striking clinical phenomena in affective disorders is its periodicity – ranging from seasonal, as in winter depression, to rapid cycling [3] (fig. 2), which can be as short as 48 h. Other periodic phenomena are found at the symptom level: diurnal variation of mood, early morning awakening and sleep disturbances....