![]()
Chapter 8
Pinamonti M, Zanconati F: Breast Cytopathology. Assessing the Value of FNAC in the Diagnosis of Breast Lesions.
Monogr Clin Cytol. Basel, Karger, 2018, vol 24, pp 68–93 (DOI: 10.1159/000479769)
______________________
Invasive Carcinoma
Invasive breast cancer is the most common carcinoma in women, accounting for 23% of all cancers worldwide [Ferlay et al., 2008]. Its incidence increases with age and varies markedly in different geographical areas due to different lifestyles and genetic factors. Australia, Europe, and North America are the regions with the highest incidence, where 6% of women develop invasive breast cancer before 75 years of age. Although it is a widespread disease, patient prognosis is usually good when it is discovered at an early stage. Nevertheless, some subtypes of breast carcinoma behave in a very aggressive way regardless of their size. FNAC is able to identify most breast cancers with high accuracy, and there are also grounds for its routine use in the molecular and genetic characterization of tumor cells without resorting to more invasive techniques [see Chapter 11, this vol., pp. 108–111].
This chapter illustrates the main forms of breast cancer, setting the basis for the diagnosis of malignancy on FNAC and providing some hints to direct the cytological interpretation towards one or the other specific type of carcinoma.
Invasive Ductal Carcinoma and High-Grade Ductal Carcinoma in situ
Introduction/Epidemiology
Invasive ductal carcinoma of no special type (NST) is the prototype of breast cancer and accounts for approximately 40–75% of all invasive carcinomas in published series, with a wide range of variation based mostly on the strictness of the criteria used for inclusion in the other “special” types [Lakhani et al., 2012]. It is actually a heterogeneous category gathering all the invasive epithelial neoplasms lacking the characteristics to be diagnosed as a specific histological type, such as tubular or lobular. The epidemiology of ductal carcinoma NST reflects the general distribution of the breast cancer group as a whole, being rare in women younger than 40 years without a familiar or genetic predisposition and increasing in incidence with advancing age. Invasive ductal carcinomas are part of a multifocal lesion in approximately 20% of cases.
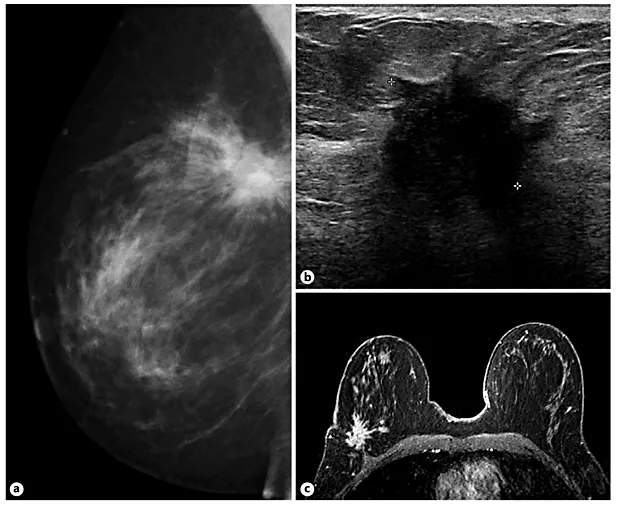
Invasive ductal carcinoma can be seen on mammography as an opacity with irregular, stellate, or nodal configuration and moderately or ill-defined contours, commonly showing calcifications. Ultrasound typically shows a hypoechoic mass with irregular shape, spiculated, indistinct, or microlobulated margins and posterior acoustic shadowing or enhancement (Fig. 1) [Blaichman et al., 2012]. Lesions larger than 2 cm, or even smaller if localized superficially or in a small breast, are often palpable and clinically detected as hard nodules. Advanced tumors may drastically alter the breast consistency and appearance, cause skin and nipple retraction or ulceration, and eventually result in the dramatic clinical presentation of inflammatory carcinoma, resembling acute mastitis.
Fig. 1. Imaging of invasive ductal carcinoma. This lesion is located in the upper-outer quadrant of the right breast and is visible as a stellate opacity on mammography (a). Ultrasound shows a hypoechoic lesion with irregular borders and posterior acoustic shadowing (b). The lesion is highly suspicious also on magnetic resonance imaging (c).
High-grade ductal carcinoma in situ (DCIS) is a noninvasive neoplastic proliferation of ductal cells characterized by marked cytological atypia and frequently by the presence of necrosis and calcifications. Pure DCIS was considered a rare entity in the past, but, recently, its incidence has increased from 4 to nearly 25% of all breast malignancies, since the more widespread introduction of mammographic screening [Patnick, 2010]. Indeed, DCIS seldom gives rise to a palpable mass and does not generate a desmoplastic reaction, so it can only be detected by mammography in the presence of coarse, pleomorphic, and branched microcalcifications. The lack of both a palpable mass and an ultrasound-detectable nodule renders a subsequent FNAC unlikely and makes other diagnostic techniques more suitable, such as vacuum-assisted core needle biopsy under stereotaxic guidance [Jackman and Rodriguez-Soto, 2006].
Histological Features
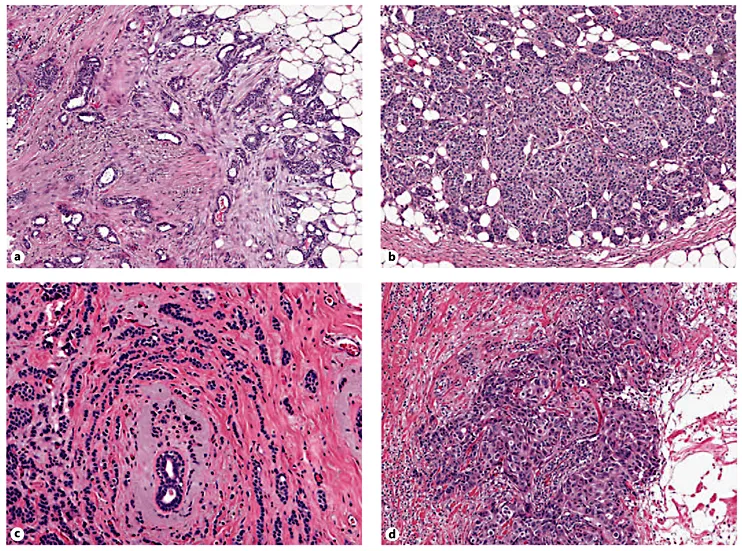
Invasive ductal carcinoma NST may show a variety of morphological aspects encompassing different degrees of cell differentiation and architectural patterns. The tumor cells may be arranged in tubular structures, cords, clusters, or trabeculae, or occasionally infiltrate the surrounding stroma in single-cell-thick Indian files (Fig. 2). Cells may have abundant eosinophilic or scant cytoplasm, and nuclei can be regular and uniform or highly pleomorphic with prominent, multiple nucleoli. Mitotic activity may be virtually absent or extensive. The modified Bloom-Richardson-Elston grading system (also called the Nottingham system) can be used to classify invasive ductal carcinomas into 3 grades of differentiation that correlate with their aggressiveness [Elston and Ellis, 1991]. It is based on architectural criteria (rate of tubule formation/resemblance to normal breast gland), combined with cytological features (nuclear atypia), and the mitotic index. Intratumor necrosis, desmoplastic reaction, and chronic inflammation are variably present in invasive ductal carcinomas and have a lesser role in defining its prognosis.
Fig. 2. Histological aspects of invasive ductal carcinoma. Well-differentiated ductal carcinomas are composed predominantly of tubular and acinar structures lined by a single layer of cuboidal cells lacking the myoepithelial component, immersed in a desmoplastic stroma (a). Moderately differentiated carcinomas may have a solid/trabecular architecture (b) or grow in single cells that infiltrate the stroma and surround normal ducts creating a sort of “target” image (c). Poorly differentiated cancers have solid architecture and show marked cellular atypia (d). H&E. Low power.
Immunohistochemistry is necessary to determine the prognosis and response of invasive ductal carcinomas NST to treatment. Hormonal receptors (estrogen and progesterone) are positive in 70–80% of cases, while human epithelial growth factor receptor 2 (HER2) is overexpressed in approximately 15% of all invasive ductal carcinomas NST [Lakhani et al., 2012].
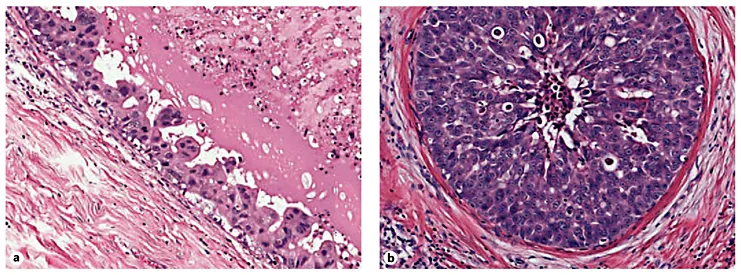
High-grade DCIS is a proliferation of markedly atypical neoplastic cells lining the walls of breast milk ducts that may have a solid, cribriform, papillary, or micropapillary configuration. The term comedo is used for high-grade DCIS showing abundant necrotic debris in duct lumina (somewhat like skin blackheads or comedones), which may calcify (Fig. 3). Unlike the low-grade form, high-grade DCIS shows pleomorphic and poorly polarized nuclei with irregular contours, coarse, and clumped chromatin, and prominent nucleoli. In a considerable percentage of cases, high-grade DCIS is associated with an invasive component [Lakhani et al., 2012].
Fig. 3. High-grade ductal carcinoma in situ (DCIS). The lesion is composed of markedly atypical cells confined to the basal membrane and may show different architectural patterns: small projections of cancer cells without fibrovascular cores characterize the micropapillary variant of DCIS (a), while comedo DCIS is made up of solid nests with necrotic material in the center (b). H&E. Intermediate power.
Cytology
The cellular material aspirated from invasive ductal carcinoma NST is typically polymorphic, showing cells with differently shaped nuclei, which can vary in size from 1.5 to 2 times the diameter of a red blood cell to even 5 times that size. Neoplastic elements are arranged in loosely cohesive monolayers or in 3-dimensional aggregates with irregular distribution and overlapping of nuclei (Fig. 4). Occasional tubular or acinar structures may be present, especially in well- or moderately differentiated cancers (Fig. 5). Myoepith...