eBook - ePub
Atlas of Equine Ultrasonography
Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer, Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer
This is a test
Compartir libro
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Atlas of Equine Ultrasonography
Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer, Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
The only visual guide to equine ultrasonography based on digital ultrasound technology. Atlas of Equine Ultrasonography provides comprehensive coverage of both musculoskeletal and non-musculoskeletal areas of the horse. Ideal for practitioners in first opinion or referral practices, each chapter features normal images for anatomical reference followed by abnormal images covering a broad range of recognised pathologies. The book is divided into musculoskeletal, reproductive and internal medicine sections and includes positioning diagrams demonstrating how to capture optimal images. With contributions from experts around the world, this book is the go-to reference for equine clinical ultrasonography.
Key features include:
- Pictorially based with a wealth of digital ultrasound images covering both musculoskeletal and non-musculoskeletal areas and their associated pathologies.
- Each chapter begins with a discussion of normal anatomy and demonstrates how to obtain and interpret the images presented.
- A video library of over 50ultrasound examinations is available for streaming or download and viewing on-the-go. Access details are provided in the book.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Atlas of Equine Ultrasonography un PDF/ePUB en línea?
Sí, puedes acceder a Atlas of Equine Ultrasonography de Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer, Jessica A. Kidd, Kristina G. Lu, Michele L. Frazer en formato PDF o ePUB, así como a otros libros populares de Medicine y Equine Veterinary Science. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Información
SECTION 1
Musculoskeletal
CHAPTER ONE
Ultrasonography of the Foot and Pastern
1University of Pretoria, Onderstepoort, South Africa
2The Royal Veterinary College, North Mymms, Hatfield, UK
The Foot
Lameness associated with the foot is common and routinely evaluated using radiography. However, many causes of lameness are associated with soft tissue pathology where there are no or minimal radiographic changes. While magnetic resonance imaging (MRI) has become the imaging modality of choice for identifying such soft tissue causes, MRI is costly and not always available. Therefore, ultrasonography is a logical imaging modality to consider but its use is compromised by the presence of the hoof capsule, which precludes imaging through it. However, there are three ultrasonographic windows where images can be obtained of structures of the foot – proximal to the coronary band palmarly and dorsally, and transcuneally/transsolarly.
Ultrasonography Proximal to the Coronary Band
A number of structures within the foot extend proximal to the coronary band and so lend themselves to ultrasonographic examination.
Preparation
The hair should be clipped and cleaned as for other ultrasound examinations. Gel should be rubbed it the area and left for a few minutes to improve contact as this is often limiting.
Technique
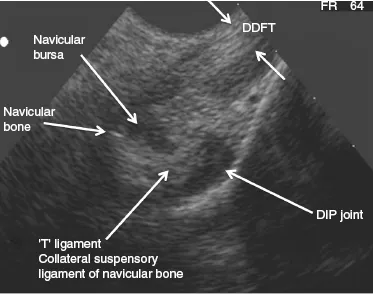
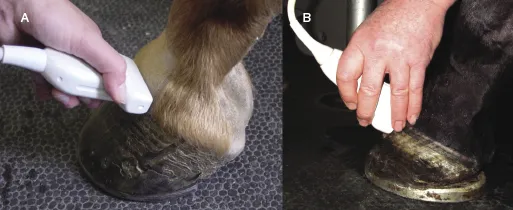
For the palmar aspect of the foot a small footprint transducer (ideally a curvilinear probe) can be placed longitudinally between the bulbs of the heel, with the foot placed on a wooden wedge (as used for foot radiography – Figure 1.1) so as to have the fetlock partially flexed and the foot extended. This allows the assessment of the deep digital flexor tendon (DDFT), the palmar pouch of the distal interphalangeal (DIP) joint, the “T” ligament, and the navicular bursa down to the level of the proximal border of the navicular bone (Figure 1.2). However, the DDFT is off-incidence to the ultrasound beam and hence is hypoechoic, and the imaging window incorporates only the middle portion of the DDFT, making identification of DDFT tears, most commonly present in the lobes, difficult.

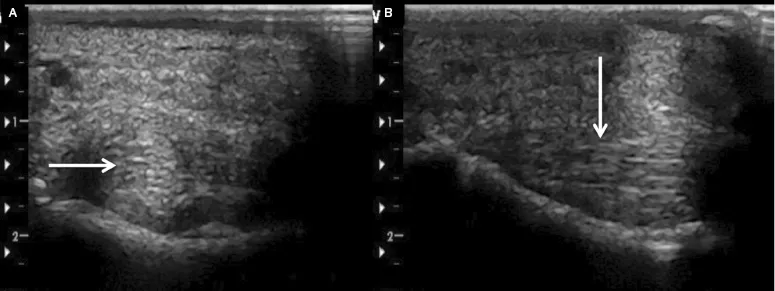
For the dorsal, medial, and lateral aspects, the transducer is positioned both transversely adjacent to the coronary band and longitudinally overlying the coronary band (Figure 1.3) and moved from the dorsal aspect to the dorsomedial and dorsolateral aspects where the dorsal joint capsule and collateral ligaments of the DIP joint (Figure 1.4) can be imaged immediately proximal to the coronary band. The collateral ligaments traverse the coronary band and so only the more proximal parts of the ligament are visible ultrasonographically. Care should be taken to ensure the transducer is on-incidence to the collateral ligament as it is easy to generate off-incidence artifacts in the ligaments that can resemble pathology (Figure 1.5). Further caudally lie the collateral cartilages, which are hypoechoic but can show areas of ossification (and therefore acoustic shadowing).
Ultrasonographic Abnormalities
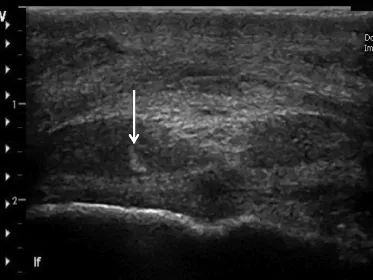
Via the palmar window, only chronic DDFT pathology, where there is retained echogenicity and/or mineralization within the off-incidence hypoechoic DDFT, can usually be visualized (Figure 1.6), limiting this view for comprehensive evaluation of the DDFT in this region of the foot. In some cases, DDFT pathology will extend sufficiently proximally to be visible in standard views within the distal pastern (see Pastern, later in this chapter).
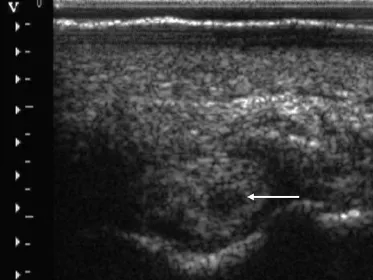
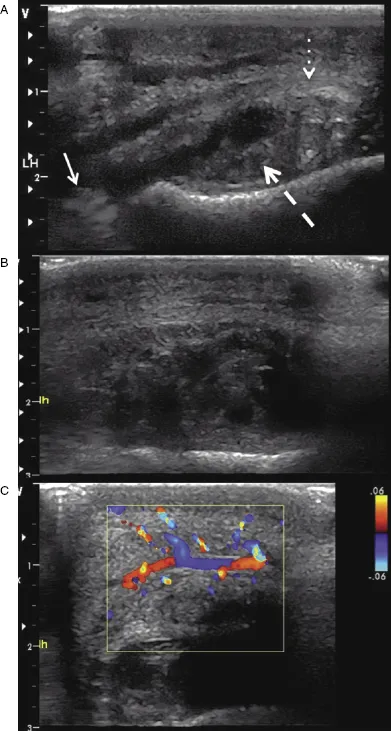
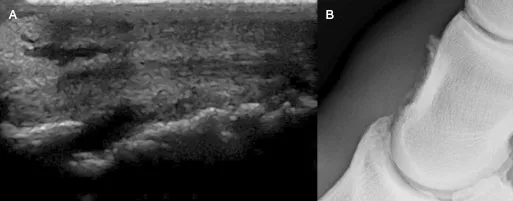
Abnormalities of the distal interphalangeal joint can result in changes to the dorsal pouch which are visible ultrasonographically – both distension and synovial thickening (Figure 1.7) as well as osteophytosis in cases of osteoarthritis (Figure 1.8). Where ultrasonography of this region carries the most useful imaging is for collateral ligament desmitis, especially when there is palpable swelling in the region of the ligament (dorsomedially or dorsolaterally) at the level of the coronary band. Ultrasonographic abnormalities vary between enlargement and complete rupture (Figure 1.9).
Transsolar and Transcuneal Ultrasonography
The third phalanx (P3), distal sesamoid bone (navicular bone) (DSB), navicular bursa (NB), implantation of the deep digital flexor tendon (DDFT), distal sesamoid impar ligament (DSBIL),...