![]()
Part I
Nuts and bolts
The first section of this book deals with two fundamental aspects of anaesthetic practice: the airway and vascular access.
General anaesthesia has been summarised by the simple phrase put up a drip, put down a tube and give plenty of oxygen. Although many anaesthetists resent this glib description of their work, it does have the virtue of emphasising the importance of venous cannulation and control of the airway, which are essential for the safe conduct of anaesthesia. Difficulties arise in anaesthesia when one of these fundamental areas is not secure, and if both fail then disaster is close at hand.
Therefore, in the first 10 chapters we concentrate on evaluation and control of the airway, the anaesthetic machine and circuits, basic anaesthetic monitoring, vascular access, and the choice of intravenous fluids. We have not given detailed instructions on how to undertake the practical procedures.
There is no substitute for careful instruction from a senior anaesthetist as part of the anaesthetic procedure. At the start of training the application of physiology and pharmacology to anaesthesia is exciting, and knowledge of the equipment may seem mundane and even boring.
It is imperative that you have a basic understanding of the equipment you use – failure to do so will put the patient at risk.
![]()
Chapter 1
Evaluation of the airway
Experienced anaesthetists teach that there are three fundamental aspects to safe anaesthetic practice: the airway, the airway and the airway. Unanticipated airway problems account for about 40% of overall anaesthetic morbidity and mortality. Tracheal intubation is now undertaken less often, mainly because of the advent of supraglottic airways such as the laryngeal mask. However, tracheal intubation remains the gold standard for airway management, control and protection. It may be required during the course of an anaesthetic or for the management of an unconscious patient. Therefore, careful airway assessment must be undertaken. This is carried out logically, as summarised in Box 1.1.
Box 1.1 Assessment of the airway
- History
- Symptoms
- Examination
- anatomy and variants
- medical conditions
- specific assessment
- Mallampati scoring system
- thyromental distance
- sternomental distance
- other tests
1.1 History
Any previous anaesthetic history must be obtained. Information about difficulties with tracheal intubation may be found in old anaesthetic records. Previous successful intubation is not an indicator of its ease. Some patients carry letters or wear MedicAlert bracelets stating their anaesthetic difficulties, while others with major problems know nothing about them. Ascertain whether the airway is potentially difficult by checking whether the patient has any of the medical and surgical conditions listed in Box 1.2.
Box 1.2 Medical features of difficult airway intubation
- Congenital: rare
- Acquired
- traumatic: fractures of mandible and cervical spine
- infection: epiglottitis, dental or facial abscess
- endocrine: thyroid enlargement, acromegaly, obesity
- neoplasia: tongue, neck, mouth, radiotherapy
- inflammatory: ankylosing spondylitis, rheumatoid arthritis
- pregnancy
1.2 Symptoms
Upper airway obstruction may be found in patients with stridor, dysphagia and hoarseness.
1.3 Examination and clinical tests
Normal anatomy and its variants
Some patients appear anatomically normal and yet are difficult, or impossible, to intubate. These patients cause anaesthetists unexpected problems. We have had the occasional experience of casually starting an apparently normal laryngoscopy, only to have the sinking feeling associated with complete failure to see the larynx. It is much better to anticipate a difficulty than encounter one unexpectedly. Some anatomical factors that make airway control and intubation difficult are listed in Box 1.3.
Box 1.3 Anatomical features of difficult airway control and intubation
- Short immobile neck
- Full set of teeth, buck teeth
- High arch palate
- Poor mouth opening – less than three fingers gap between upper and lower teeth
- Receding mandible (may be hidden by a beard)
- Inability to sublux the jaw (forward protrusion of the lower incisors beyond the upper incisors)
Specific assessment
Several clinical tests to assess the airway are in common use. None is reliable in predicting a difficult airway or intubation, and all should be used in combination as this provides a better overall assessment of the airway.
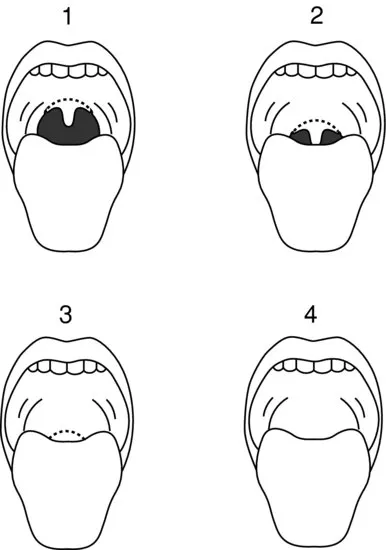
Modified Mallampati scoring system
This predicts about 50% of difficult intubations. The test can be performed with the patient in the upright or supine position. It is based upon the visibility of the pharyngeal structures with the mouth open as wide as possible (Figure 1.1). Patients are classified as follows:
- Grade 1: faucial pillars, soft palate and uvula visible
- Grade 2: faucial pillars, soft palate visible, but uvula masked by the base of the tongue
- Grade 3: soft palate only visible
- Grade 4: soft palate not visible
Patients in grades 3 and 4 are considered difficult to intubate, and those in grades 1 and 2 are considered feasible intubations. It is important to realise that this system is not infallible, and patients in grade 2 sometimes cannot be intubated.
Head and neck movement
Flexion and extension are greater than 90° in normal people.
Jaw movement and mandible
Check that the patient's mouth opens normally. It should have an interincisor gap of greater than 5 cm (about three finger breadths). Check that the patient does not have buck teeth or a receding mandible. Ideally, the lower incisors should be able to be protruded beyond the upper incisors. If these simple tests cannot be performed the airway may be difficult to manage.
Thyromental distance
The thyromental distance (Patil test) is the distance from the thyroid cartilage to the mental prominence when the neck is extended fully (Figure 1.2). In the absence of other anatomical factors, if the distance is more than 6.5 cm, problems should not occur w...