Inside today's data-driven personalized medicine, and the time, effort, and information required from patients to make it a reality Medicine has been personal long before the concept of “personalized medicine” became popular. Health professionals have always taken into consideration the individual characteristics of their patients when diagnosing, and treating them. Patients have cared for themselves and for each other, contributed to medical research, and advocated for new treatments. Given this history, why has the notion of personalized medicine gained so much traction at the beginning of the new millennium? Personalized Medicine investigates the recent movement for patients’ involvement in how they are treated, diagnosed, and medicated; a movement that accompanies the increasingly popular idea that people should be proactive, well-informed participants in their own healthcare. While it is often the case that participatory practices in medicine are celebrated as instances of patient empowerment or, alternatively, are dismissed as cases of patient exploitation, Barbara Prainsack challenges these views to illustrate how personalized medicine can give rise to a technology-focused individualism, yet also present new opportunities to strengthen solidarity. Facing the future, this book reveals how medicine informed by digital, quantified, and computable information is already changing the personalization movement, providing a contemporary twist on how medical symptoms or ailments are shared and discussed in society. Bringing together empirical work and critical scholarship from medicine, public health, data governance, bioethics, and digital sociology, Personalized Medicine analyzes the challenges of personalization driven by patient work and data. This compelling volume proposes an understanding that uses novel technological practices to foreground the needs and interests of patients, instead of being ruled by them.
Domande frequenti
Come faccio ad annullare l'abbonamento?
È semplicissimo: basta accedere alla sezione Account nelle Impostazioni e cliccare su "Annulla abbonamento". Dopo la cancellazione, l'abbonamento rimarrà attivo per il periodo rimanente già pagato. Per maggiori informazioni, clicca qui
È possibile scaricare libri? Se sì, come?
Al momento è possibile scaricare tramite l'app tutti i nostri libri ePub mobile-friendly. Anche la maggior parte dei nostri PDF è scaricabile e stiamo lavorando per rendere disponibile quanto prima il download di tutti gli altri file. Per maggiori informazioni, clicca qui
Che differenza c'è tra i piani?
Entrambi i piani ti danno accesso illimitato alla libreria e a tutte le funzionalità di Perlego. Le uniche differenze sono il prezzo e il periodo di abbonamento: con il piano annuale risparmierai circa il 30% rispetto a 12 rate con quello mensile.
Cos'è Perlego?
Perlego è un servizio di abbonamento a testi accademici, che ti permette di accedere a un'intera libreria online a un prezzo inferiore rispetto a quello che pagheresti per acquistare un singolo libro al mese. Con oltre 1 milione di testi suddivisi in più di 1.000 categorie, troverai sicuramente ciò che fa per te! Per maggiori informazioni, clicca qui.
Perlego supporta la sintesi vocale?
Cerca l'icona Sintesi vocale nel prossimo libro che leggerai per verificare se è possibile riprodurre l'audio. Questo strumento permette di leggere il testo a voce alta, evidenziandolo man mano che la lettura procede. Puoi aumentare o diminuire la velocità della sintesi vocale, oppure sospendere la riproduzione. Per maggiori informazioni, clicca qui.
Personalized Medicine è disponibile online in formato PDF/ePub?
Sì, puoi accedere a Personalized Medicine di Barbara Prainsack in formato PDF e/o ePub, così come ad altri libri molto apprezzati nelle sezioni relative a Medicine e Health Care Delivery. Scopri oltre 1 milione di libri disponibili nel nostro catalogo.
When proponents of personalized medicine explain the concept, they typically tell a story of technological progress. Medicine used to be hit-and-miss, they say. We used to treat all people with a certain disease the same, despite all their differences. With today’s technological tools we have become much better at measuring individual difference. Personalized medicine—especially in its iteration of precision medicine, which seeks to include ever wider types of information and monitoring—is the future. It is time to say farewell to “blockbuster medicine.”
This future has already started. The idea that medicine and health care should become personalized—in the sense that they should be tailored more closely to individual characteristics of patients—has entered almost every domain of health care. Let us take the example of Type-1 diabetes, which is a relatively common disease. In the United States and in Europe, about two to three in a thousand people are affected by it, most of them at a young age (Menke et al. 2013; Patterson et al. 2009). Historically, the prevalence of diabetes has been highest among European populations, but now it is on the rise also in low- and middle-income countries. In contrast to Type-2 diabetes, which has been known as “adult onset diabetes” and can often be managed by diet and exercise, most Type-1 diabetes patients rely on insulin injections. Before the discovery of insulin treatment in the 1920s, Type-1 diabetes sufferers were put on so-called starvation diets. Fasting and restricted food intake, it was believed, could prolong the lives of patients. Despite this, many patients died within months of the diagnosis.
After the introduction of insulin treatment, the tools required consisted of a simple finger prick set to determine glucose levels, and a syringe to inject insulin. Then, in the late twentieth and early twenty-first century, companies developed more complex monitoring and treatment systems, including microchip sensors, automated insulin pumps, and insulin inhalers. Today, “smart socks” can measure changes in temperature in patients’ feet to detect inflammation that could lead to foot ulcers, which affect many diabetes sufferers. And insulin meters can send text messages to parents about their child’s glucose levels. Patients in high-income countries are encouraged to use these tools to tailor their diabetes treatment more closely to their individual needs. Every diabetes sufferer is different, so the story goes, and monitoring blood glucose within very narrow ranges with the help of close monitoring leads to better health outcomes—at the cost of five hundred dollars per month or more, with treatment tools and insulin increasing in quality and price.
Another example of the personalization of diagnosis and treatment is the molecular classification of tumors. It is well known by now that the treatment of breast cancer can be improved by looking at the specific characteristics of the tumor. But this practice is not restricted to breast cancer alone. Glioblastoma multiforme (GBM), for example, is a rare but very aggressive brain cancer. Its prevalence is not known exactly because it remains undiagnosed in many resource-poor regions. In high-income countries, it is estimated that GBM makes up about 15 percent of all brain tumors. Once diagnosed, most patients die within three years. GBM tumors are resistant to conventional therapies, and treatment options vary depending on the tumor’s location. For a long time, surgery, chemotherapy, radiation, and palliative treatment were the only options available. More recently, gene transfer has been explored as an additional treatment option, and promising results were achieved with the use of a nonpathogenic version of an oral poliovirus type in clinical trials at Duke University (Gromeier 2018). Moreover, factors such as the precise location of the tumor, patient age, and molecular markers such as the concentration of certain growth factors allow probabilistic inferences regarding treatment response and survival rates. The molecular classification of tumors is thus seen as a way to more individualized therapies that “will ideally lead to better outcomes in both the quantity and quality of life” (Choudhry et al. 2013: 303).
Is personalized medicine the crown of the evolution of medicine? Is it a step toward truly individualized medicine, and is the latter something that we should strive for? While many advocates of personalized medicine would answer these questions with a resounding yes, others are less enthusiastic. They remind us that medicine has long been personalized. Physicians, nurses, and carers have always considered the individual characteristics and circumstances of their patients when diagnosing, treating, and caring for them (Hunter 1991). In the days before professionalized medicine, and certainly before medicine’s reliance on instruments that only trained professionals could operate, patients played a key role in medical decision making processes: Their stories and descriptions of symptoms were often indispensable for determining diagnosis. Patients and their families have also participated in deciding on and administering care (see also Strauss et al. 1982; 1997). Historically, “bedside medicine,” with its close interactions between patients, doctors, and families and with its consideration of the specific circumstances and experiences of the patient, has been the rule, and not the exception.
If we accept that medicine has always been personalized, why is it, then, that the concept of personalized medicine has received so much traction recently? Is there anything new about the kind of personalized and “precision” medicine that is the topic of policy papers, funding calls, and government initiatives today? Although I agree that we should be cautious not to celebrate personalized medicine as an entirely novel phenomenon, it is clear that several developments within the last two decades have changed the institutions, practices, and stakes of medicine. The spread of digital technologies and the “biomarkerization” (Metzler 2010) of medicine—that is, the increasing reliance on objectively measurable somatic markers representing specific stages of physiology and pathology—have changed the meaning of evidence that is used to personalize medicine. In the 1960s, the British novelist Peter Berger portrayed the life of an English country doctor. For decades to come, his book was on the reading list of people training to become doctors. In order to recognize a patient’s illness, Berger noted, doctors “must first recognize the patient as a person” (Berger and Mohr 1967: 76). In other words, doctors, when assessing the likely cause and nature of a disease, need to consider wider ranges of factors than the immediate symptoms that a person presents with. This statement is very similar to the slogans of proponents of personalized medicine today: The U.S. Precision Medicine initiative, for example, explores how genes, environment, and lifestyle come together to create a “unique thumbprint” of each patient (National Institutes of Health 2016a). What has changed is thus not the commitment to focus on individual characteristics of patients but the very characteristics that should be considered. When diagnosing and prescribing treatments, Berger’s country doctor considered the living circumstances of his patients, their family and social relationships, and their mental state. These were all aspects that doctors who still made house calls used to know—or explore in a dialogue with their patients. Within contemporary personalized medicine, it is a person’s genetic predispositions, her lifestyle information, and clinical data that should be brought together into personal health maps informing diagnosis and treatment. It is no longer unstructured narrative information that is seen as the key to personalization, but structured, digital, quantified, and computable data (see also Hartzband and Groopman 2016; de Mul 1999; Nettleton 2004; Webster 2002).
Another push toward such a new understanding of evidence has come from the advance of high-throughput technologies—the devices and computational tools that enable the simultaneous examination of large amounts of genes, proteins, and metabolites. A standard reference in this context is Moore’s Law, named after Intel founder Gordon Moore; it predicts that the number of transistors on integrated computer circuits doubles every two years (G. Moore 1965). The cost of sequencing a human genome—the sum of a person’s DNA—has decreased faster in the last decade than predicted even by Moore’s Law. At the same time, the speed of analysis has increased drastically (National Human Genome Research Institute 2014). Advances in the production of data on gene expression, blood glucose levels, or brain function, for example, have contributed to a situation in which Western biomedicine is now faced with unprecedented amounts of digital data. Finding a way to transform these data into something meaningful and, if possible, clinically actionable, is one of the main challenges that clinicians, patients, enterprises, and health authorities struggle with.
In policy papers, politicians’ speeches, and newspaper articles today, personalization appears as the data-intense characterization of individuals at different stages of health and disease in the course of their lifetime. This is different from how the term was understood in the 1990s and early 2000s, when personalized medicine largely meant tailoring drug treatments to genetic characteristics of population sub-groups (Hedgecoe 2004). Today’s vision of personalization seeks to make use of much wider ranges of molecular and nonmolecular data and information, including imaging data, information about lifestyle and diet, and records of physical examinations (European Science Foundation 2012; PerMed Consortium 2015; Weber, Mandl and Kohane 2014). This is also how I use the term personalized medicine in this book. I understand precision medicine (National Research Council of the Academies 2011; see also Juengst et al. 2016) and stratified medicine1 as variants of the idea that I subsume under the generic label of personalization.
Where Patients Come In: The “Google Maps” of Health Data
Former U.S. President Obama made personalized medicine prime time news when he announced the allocation of $215 million to the study of “individual differences in people’s genes, environment and lifestyle” in his State of the Union address in 2015 (White House 2015). He referred to this new type of medicine as precision medicine. The paradigmatic vision of precision medicine was first formulated in a report by the Committee on a Framework for Developing a New Taxonomy of Disease within the U.S. National Academies of Sciences in 2011 (National Research Council of the Academies 2011). The report proposed to replace traditional, symptom-based disease classifications with a new taxonomy based on data-rich characterizations of individuals and disease states. The report used the “Google Maps” feature, with its different layers of data—including data on transportation, land use, and postal codes—as a template for what a new map of patient-centered information could look like. The report’s vision was that this map should serve both clinical and research needs (17). In such a system of patient-centered data, genetics may still play the first violin in some contexts, but it is part of a bigger orchestra.
But where do the data for such a personalized health data map come from? Many kinds of nonmolecular data that are envisaged to be part of such a health-data system—including information about the details of a person’s lifestyle, mood curves, or data from the daily tracking of functional changes following the start of a new medication—are not readily available from clinical or biomedical research contexts. Some of the data would need to come from other, non-biomedical research contexts, remote sensors, or people’s personal domains.
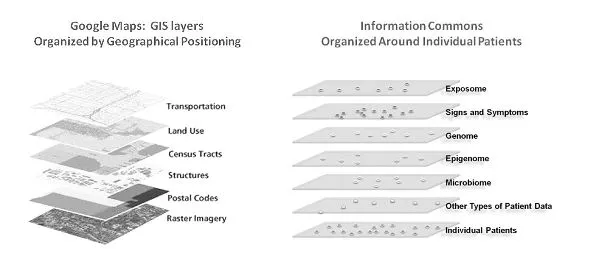
Figure 1.1. An Information Commons might use a GIS-type structure. The proposed, individual-centric Information Commons (right panel) is somewhat analogous to a layered GIS (left panel). In both cases, the bottom layer defines the organization of all the overlays. However, in a GIS, any vertical line through the layers connects related snippets of information since all the layers are organized by geographical position. In contrast, data in each of the higher layers of the Information Commons will overlay on the patient layer in complex ways (e.g., patients with similar microbiomes and symptoms may have very different genome sequences). Source: FPA (Fire Program Analysis) 2011, GIS Overview, FPA Project, Idaho State Office, Bureau of Land Management, Boise, ID, www.fpa.nifc.gov, accessed August 19, 2011 (left panel); screenshot from Insel 2011 (right panel). Reprinted with permission of the National Institute of Mental Health. Original caption was retained.
Since the report was published, the “Google Maps for health” metaphor has become a trope, popularized also by physician researcher and author Eric Topol’s use of the comparison between geographical information systems and personal health maps (Topol 2015). Topol argues that in the near future, personal health maps will enable patients to carry out most diagnoses themselves. Even visionaries and practitioners who do not believe that algorithmically supported patients will take over the role of doctors any time soon see the integration of diverse types of data sets as crucial for the realization of personalized medicine. And they agree that this goal, in turn, will depend on the willingness of people to participate in the generation and analysis of data.
Many technologies to help patients with this task are already here. Touch-screen-fitted and portable devices make it technically easier to collect and transfer data and information. Websites and platforms “pull” data from users seeking to access information on the Internet—often without their being aware of what it is they are contributing (Wellcome Trust 2016). In other words, the Internet2 has ceased to be primarily a provider of information and has become a tool for data collection from patients and citizens (Kallinikos and Tempini 2014; Prainsack 2013; Tempini 2015). Data that were not previously considered relevant in the health care context—such as mood-tracking data stored on smart phones—are now seen as potentially useful resources. Viktor Mayer-Schönberger, an information governance expert, and Kenneth Cukier, an editor at The Economist, use the term “datafication” to refer to this process. According to these authors, we are taking “information about all things under the sun—including ones we never used to think of as information at all, such as a person’s location, the vibrations of an engine, or the stress on a bridge—and transforming it into a data format to make it quantified” (Mayer-Schönberger and Cukier 2013: 15).
That increasing parts of our lives, bodies, and environments are “datafied” does not mean that these data can always be integrated and interpreted in a meaningful way. Improving the interoperability between different data sets and data repositories, data integration, and quality control at the point of data entry remains a difficult challenge, despite promising attempts of tech developers. But here, too, it is apparent that these challenges cannot be addressed without active participation by patients who are needed to collect, hand over, or help analyze data and information.
The central role of patients in personalized medicine was apparent also in Barack Obama’s vision: collaborative health care and “patient-powered” research form central pillars of the U.S. Precision Medicine Initiative (White House 2015). With this emphasis on patient-centered personalized medicine, the United States is not alone: Proponents of personalized medicine around the world believe that it can kill two birds with one stone: to render medicine more effective and, at the same time, “empower” patients.
Whom Does Personalized Medicine Empower?
But are patients “empowered” by personalized medicine? Social scientists who have been studying twentieth- and twenty-first-century versions of personalization in medicine draw a nuanced picture. Sociologist Richard Tutton, for example, grounds his analysis in the sociology of expectations, which treats speculative claims about the future of a field of science or technology as “fundamental to the dynamic processes that create new socio-technical networks” (Hedgecoe and Martin 2003: 328). In other words, visionary statements about the development of a field often create facts on the ground. In the case of personalized medicine, Tutton argues, the notion serves to overturn the fiction of the standard patient (Tutton 2012; 2014). The idea that every disease was marked by a list of specific characteristics and symptoms that all patients in this group would typically display was a central theme within the scientific ideal of Western medicine in the nineteenth century. The current version of personalized medicine, in contrast, draws attention to the innumerable differences between patients and the ways in which their diseases affect them. It highlights the ways in which the same disease develops and expresses itself differently between people, due to differences in lifestyle, diet, genetic makeup, and so forth. In fact, the more we know about differences between people in molecular, lifestyle, and other terms, the farther we get away from the notion that any two people express the same disease in the same way (European Science Foundation 2012; Harvey et al. 2012). In its extreme form, personalized medicine means that there are as many diseases as there are people. Diseases could still be bundled together in clusters that display similarities, but the idea of common disease labels would be obsolete (National Research Council of the Academies 2011; Prainsack 2015a).
Tutton argues that this discursive and technological shift draws attention away from social determinants of health toward an illusion of a technological fix for health problems in our societies. In such a context, personalized medicine appears as an overhyped idea that benefits companies and uses the notion of risk to enlist patients in governing themselves more effectively (Tutton 2014; see also Tutton and Prainsack 2011). Similarly, Donna Dickenson, in her book Me Medicine vs. We Medicine (2013), sees personalized medicine as a political rhetoric that makes people believe that it is good for them, while it is really driven by corporate interests and fosters questionable values such as ruthless individualism. Also other critical authors consider the main function of the concept of personalized medicine to be a political one: They see it as diverting attention away from the failure of big science and heroic medicine to make a tangible difference for people’s health (Nuffield Council on Bioethics 2010). This diversion is achieved by implying a shift “from industrial mass production to targeted fabrication” (Prainsack and Naue 2006: 349), which runs the risk of reiterating racial, gender, and class biases in a more concealed way than ever (Clarke et al. 2010b; see also Prainsack 2015a).
Here, the examples of personalized diabetes management and the molecular classification of brain tumors at the beginning of this chapter are instructive. First of all, in both scenarios, key aspects of personalization are out of reach for people in low-income countries. That the majority of the world’s population will be excluded from enjoying the benefits of personalization has indeed been a key concern of critical observers (Khoury and Galea 2016). But it is not only populations in low-income countries that would be deprived of access to personalizing technologies such as blood-monitoring instruments or tumor analysis, but also less-privileged people within high-income countries. Even for people who could have access to technologies and services used to personalize their health care, social circumstances such as the lack of transportation, the fear of missing days from work, or unconscious racial bias represent factual obstacles to accessing health care, or detract from the quality of care received (Brawley and Goldberg 2012; Matthew 2015; Roberts 2011). Moreover, the increasing digitization of tasks and services—ranging from booking doctor’s appointments to using video calls for consultations to managing health records electronically—creates new patterns of exclusion. People who cannot or will ...