![]()
Chapter 1
Black CM (ed): Chlamydial Infection: A Clinical and Public Health Perspective.
Issues Infect Dis. Basel, Karger, 2013, vol 7, pp 9–24 (DOI: 10.1159/000348750)
______________________
Epidemiology and Prevention and Control Programs for Chlamydia
Catherine L. Satterwhite · John M. Douglas, Jr.
Division of STD Prevention and National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention, Atlanta, Ga., USA
______________________
Abstract
An estimated 2.9 million cases of Chlamydia trachomatis occur annually in the USA, and while most infections are not detected and reported, chlamydia is the most commonly reported nationally notifiable disease in the USA, with over 1.2 million cases reported in 2009. Rates of reported cases of chlamydia have increased over the past decade as a result of expanded use of more sensitive diagnostic tests and increased testing. The highest case rates are in adolescents/young adults, females and African-Americans. In contrast to increases in reported case rates, prevalence in routinely tested populations appears to be stable in some settings (e.g. women tested in family planning clinics) and declining in others (e.g. high-risk youths assessed by the National Job Training Program, the general population assessed by the National Health and Nutrition Examination Survey). Prevention and control programs rely on detection and treatment of infection to prevent complications and ongoing transmission, based primarily on recommended annual screening of young sexually active women and treatment of sex partners. Important complementary prevention components include enhancing awareness to promote adherence to recommended testing and education and risk reduction counseling to promote condom use. Enhancing the public health impact of chlamydia prevention and control requires expanding population coverage of recommended strategies, especially among the most affected populations.
Copyright © 2013 S. Karger AG, Basel
Current Burden of Infection
An estimated 2.9 million cases of Chlamydia trachomatis infection occur annually in the USA [1]. However, many of these infections are not detected and treated. Despite this, chlamydia is still the most commonly reported nationally notifiable disease [2]. Chlamydia was made a nationally notifiable disease in 1995 and was reported by all states by 2000. In 2009, over 1.2 million cases were reported; four times more chlamydia cases were reported than gonorrhea cases, the next most frequently reported notifiable disease [3].
Chlamydia may lead to serious adverse outcomes among women, including pelvic inflammatory disease (PID), ectopic pregnancy, tubal-factor infertility and chronic pelvic pain. Among men, chlamydia may result in urethritis, prostatitis and epididymitis. The frequency of occurrence, asymptomatic nature of infection and the possibility of adverse outcomes prompted the development of widespread screening recommendations for women in 1993 [4]. Currently, annual chlamydia screening is recommended for all sexually active women aged 25 years or younger [5]. Rates of reported chlamydia are highest among young women, reflecting these screening recommendations. Among women aged 14-19 years, the 2009 reported chlamydia rate was 3,329.3 cases per 100,000 population; among women aged 20-24, the rate was 3,273.9. Reported case rates among men are substantially lower (in 2009, 1,120.6 cases per 100,000 men aged 20-24 years). Lower reported rates in men are likely due to lower rates of testing and detection of chlamydial infections in this population, when compared to broad screening among women. Racial disparities exist in reported chlamydia rates, likely related at least in part to social determinants of health such as poverty, access to healthcare and living in communities with high STD prevalence: in 2009, black men and women were over eight times more likely than white men and women to have a reported case of chlamydia [3].
An analysis of chlamydia data from 1999 to 2002 from the National Health and Nutrition Examination Survey (NHANES), a continuous population-based survey conducted annually, showed that overall chlamydia prevalence among the general population of US men and women aged 14-39 years was 2.0% (95% confidence interval, CI, 1.6-2.5%) [6]. NHANES consists of annual data on approximately 5,000 US, noninstitutionalized men and women, selected using complex sampling methodology. Stratified by age group, chlamydia prevalence was highest among young men and women aged 20-29 years (3.2%). As with case report data, non-Hispanic blacks bore a disproportionate burden of infection with a prevalence of 5.3%, compared to a 1.5% prevalence among white men and women. The prevalence of infection was similar among men (2.0%) and women (2.5%), contrary to case reports which are more likely to reflect screening practices. In a more recent NHANES analysis limited to sexually active adolescent women aged 14-19 years, chlamydia prevalence was 7.1% [7].
Epidemiologic Trends
While estimates of chlamydial infection provide a comprehensive picture of current burden, assessing longitudinal trends are essential when considering a possible impact of prevention efforts. However, interpreting chlamydia trends is challenging. When examining trends, two important factors must be considered: changes in test technology utilization and changes in screening coverage.
Chlamydia Test Technology
Chlamydia test technology has substantially changed over time. The current optimal test technology utilized to detect genital C. trachomatis infections is a nucleic acid amplification test (NAAT) [8]. No true gold standard test for chlamydia exists; however, NAAT performance is superior to the traditional gold standard, C. trachomatis culture [9], with estimated sensitivity of greater than 90% and specificity levels of approximately 99% [8]. First introduced in the late 1990s, NAAT technology usage was initially cost prohibitive. However, as costs were reduced and additional studies demonstrated clear advancements over prior generation tests, usage increased. In 2000, 24.5% of all chlamydia tests conducted in surveyed public health laboratories in the USA were NAATs [10]; by 2007, this proportion had increased to 81.6% [11].
While improvements in test technology have been advantageous for diagnosis, they present significant challenges in determining and interpreting epidemiologic trends. The increased sensitivity of newer tests has resulted in better detection of existing infections; older test technologies likely missed infections due to reduced sensitivity [12]. If test type is not considered, increases in chlamydia rates due to use of more sensitive tests may incorrectly appear to represent increases in actual disease burden. Studies have demonstrated the impact of test technology in estimating chlamydia prevalence. Dicker et al. [12] found that chlamydia positivity in Philadelphia family planning clinics increased by 46% when NAATs replaced DNA probes (from 4.1 to 6.0%). Likewise, an analysis of data from the National Job Training Program (NJTP) revealed a 1-year increase (2005-2006) in prevalence from 9.1 to 13.9% (53% increase) associated with a dramatic shift in test technology: from 2005 to 2006, NAAT usage went from 21 to 88% of all tests [13]. When chlamydia trends were assessed, prevalence in the NJTP increased between 2003 and 2007, but after adjustment for test technology and other confounding factors, a statistically significant decrease was reported, highlighting the importance of test technology in interpreting chlamydia surveillance trends.
Chlamydia Screening Recommendations
Screening recommendations for young sexually active women have been in place since 1993 [4]. Currently, the Centers for Disease Control and Prevention (CDC) recommends that all sexually active women under the age of 26 years be screened annually for chlamydia [5]. In addition, the US Preventive Services Task Force (USPSTF) has recommended screening of young, sexually active women since 2001 [14]. In 2007, USPSTF updated their chlamydia screening recommendations to change the upper age bound from under 26 years to under 25 years of age, a change from the CDC-recommended upper age range [15] made to be consistent with nationally reported surveillance data age groupings [16]. Both CDC and USPSTF also recommend chlamydia screening for older women with risk factors. In sum, both the CDC and USPSTF, as well as most major medical organizations, uniformly recommend that young, sexually active women under the age of 25 years be screened annually for chlamydia [17].
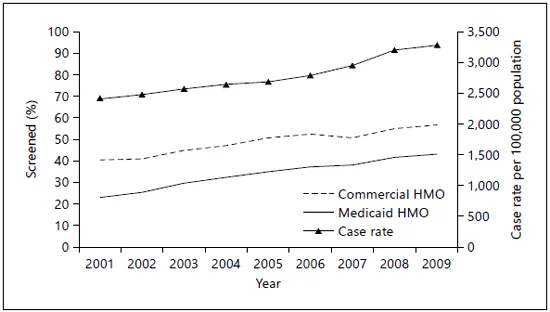
Fig. 1. Chlamydia screening coverage and chlamydia case report rates, women aged 15-24 years, 2001-2009. Sources: US national chlamydia morbidity data [C. Satterwhite, pers. commun.] and The State of Healthcare Quality, 2010 [19]. In 2001, screening coverage data are for women aged 16-26 years; from 2002-2007, women aged 16-25 years and from 2008-2009, women aged 16-24 years. Screening coverage is among women seeking healthcare who are considered to be sexually active. HMO = Health maintenance organization.
The National Committee for Quality Assurance added chlamydia screening coverage among women as a measure in the Healthcare Effectiveness Data and Information Set (HEDIS) in 1999 [18]. Chlamydia screening coverage, as measured by HEDIS, has increased steadily over time. Between 2001 and 2009, screening coverage among young women (aged 16-26 years in 2001; 16-25 years from 2002 to 2007; 16-24 years from 2008 to 2009) who were enrolled in a commercial healthcare plan and had a visit where they were determined to be sexually active increased substantially, from 23.1 to 43.1% (fig. 1) [19]. Overall, coverage was consistently higher among Medicaid populations when compared to commercial populations, and from 2001 to 2009 coverage in the Medicaid population increased from 40.4 to 56.7%. Increasing chlamydia screening coverage has undoubtedly had a substantial impact on trends in reported cases, since, as more women are screened, more existing cases are detected (fig. 1).
Epidemiologic Trends in Chlamydial Infection
For the past 20 years, reported overall chlamydia case rates (all ages, both sexes) have ...