![]()
Misra M, Toma S, Shinzato T (eds): Buttonhole Cannulation: Current Prospects and Challenges.
Contrib Nephrol. Basel, Karger, 2015, vol 186, pp 1-12 (DOI: 10.1159/000431159)
______________________
History of the Buttonhole Technique
Madhukar Misra
Division of Nephrology, Department of Medicine, University of Missouri, Columbia, Mo., USA
______________________
Abstract
The constant side method of access cannulation in hemodialysis, popularly known as the ‘buttonhole’ method, has an interesting history. Dr. Zbylut J. Twardowski, a Polish nephrologist, discovered this technique by pure serendipity in 1972. A patient with a complicated vascular access history and limited options for cannulation was repeatedly ‘stuck’ at the same sites by a nurse. Soon it was noticed that the cannulation at the same spot became easier with time. Since the needles were being reused, the sharpness of the needles decreased with time and the bluntness of the needle seemed to minimize the damage to the cannulation tract (another serendipity!). This method soon became popular among patients, and many patients started using this technique. This chapter traces the invention of this technique and its subsequent development following Dr. Twardowski’s emigration to the USA.
© 2015 S. Karger AG, Basel
Dr. Twardowski described the discovery of the ‘buttonhole’ method in his auto-biography [1]. From 1969 to 1972, all needle insertions in the Dialysis Center in Bytom, Poland, under his direction were done in different sites of the arterialized vein. In 1971, a 26-year-old lady, Maria Zieleniec-Madejska, was admitted to the center with end-stage renal disease due to chronic glomerulonephritis. She had an arteriovenous fistula created on the left radial artery and cephalic vein, but before it developed she inadvertently hit the anastomosis with a ‘Click Clack’ - a popular toy at the time. The fistula clotted, but because she needed hemodialysis immediately, she was started, on April 4, 1971, on chronic hemodialysis with an arteriovenous shunt inserted originally into the right femoral artery and femoral vein and later into the left radial artery and the left cephalic vein. In February the following year, an arteriovenous fistula was created on the right radial artery and hemodialysis was started on the fistula in March 1972. The patient had very limited segments suitable for needle insertion. Only one nurse, Sister Helena Kubara was sufficiently experienced to cannulate her fistula. Out of necessity, the insertion of needles was done repeatedly in the same spots. Within a few months the patient noted that needle insertions were not painful and requested not to use lignocaine.
After hearing about the patient’s positive experience by word of mouth, other patients requested constant-site needle insertion.
It was observed that the insertion was not painful after the track was created, was accomplished quickly, and that no complications were noted. Eventually this method came to be used in other patients. In the course of 6 months it was accepted by all 16 patients under treatment at that time. After at least a month of Sister Helena performing the technique, other nurses were in a position to cannulate fistulas. The overall results and our experience with the fistulas were published in 1977 [2]. In this paper, seemingly paradoxical observations regarding improvement of fistulas with frequent dialysis up to six times weekly were reported. As can be seen, the discovery of the constant-site method was serendipitous. Dr. Twardowski said that his role was positive in the sense that he did not reject out of hand the discovery made by a patient and a nurse. A report describing specifically the constant-site method of needle insertion was published 2 years later [3]. This paper provided a detailed comparison of different-site versus constant-site needle insertion. A comparison of 4,060 hemodialysis sessions using the different-site method and 6,180 hemodialysis sessions using the constant-site method showed the tremendous advantages of the latter method, particularly with regard to hematoma formations, reinsertions, and patient and nurse preference (table 1). There was a tendency to higher infections at the puncture sites requiring antibiotic treatment, although the difference in comparison to the different-site method was not statistically significant.
For the different-site cannulation method, very sharp needles manufactured by the Seattle Artificial Kidney Supply Co. (Seattle, Wash., USA) were used. Initially the same needles were used for the constant-site method, but they were replaced by needles manufactured by Fabryka Narzędzi Lekarskich i Dentystycznych w Milanówku (Factory of Medical and Dental Instruments in Milanówek, Poland), which were considerably less expensive. These needles were not as sharp as the needles used previously for the different-site method and were reused, which made them even blunter. The bluntness of these needles was advantageous for the constant-site method as they went through the established path without cutting adjacent tissue. New needles were used to establish the tunnel path and became blunter with reuse, so it was a smooth transition from sharp to blunt needles. It was another serendipitous discovery.
Table 1. Comparison of the two methods of needle insertion in the original study [3]
| Different sites | Constant sites |
Fistulas (n) | 22 | 25 |
Dialysis session (n) | 4,060 | 6,180 |
Time for setting up dialysis (min) | 15-25 | 5-15 |
Reinsertion (%) | 9.91 | 0.96 |
Hematoma formation (%) | 12.5 | 0.1 |
Fistula limb failure (n) | 3 | 1 |
Fistula failure (n) | 1 | 1 |
Infection requiring ABX (n) | 1 | 3 |
Patients' preference | no | yes |
Nurses'preference | no | yes |
ABX = Antibiotics. | | |
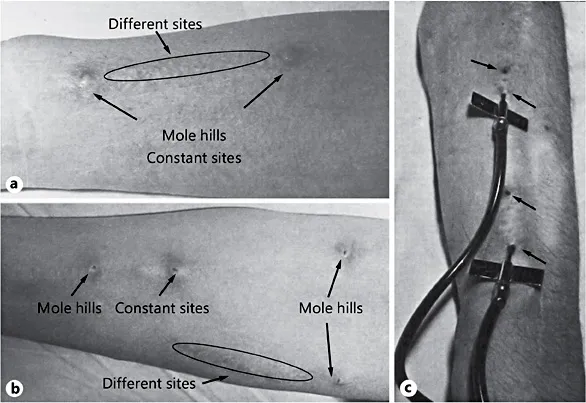
In most patients on thrice-weekly dialysis only two sites were used (fig. 1a). Some patients, however, required more than thrice-weekly dialysis, in which case there were two sites of insertion (fig. 1b, c) that were used alternately as Dr. Twardowski noted ‘insertion at the same site day after day is painful’ [3]. In 1977 Dr. Twardowski became the Chairman of the Department of Nephrology of the Medical Academy in Lublin and introduced this method where it was used in patients with Cimino-Brescia fistulas and saphenous vein grafts with the same results [3].
The decrease in the rate of hematoma formation was partly contributed to the use of antegrade insertion of the withdrawal (arterial) needle. The original suggestion of the inventors of arteriovenous fistula for hemodialysis was to direct the needle withdrawal retrograde [4]. This practice has been followed by others for many years. One of the reasons was to avoid blood recirculation during hemodialysis; however, blood recirculation does not depend on the needle direction, so there is no good reason for using a retrograde needle direction. Blood recirculation happens when the intended blood flow through the dialyzer is higher than the fistula blood flow, particularly if the needles are inserted very close to each other. In 1973, Woodson and Shapiro [5] from the Division of Thoracic Surgery and Division of Nephrology, Medical College of Ohio (Toledo, Ohio, USA), presented compelling arguments for using an antegrade direction for both needles since a retrograde direction of the withdrawal needle was associated with increased formation of hematomas and pseudoaneurysms. In the original studies on the constant-site method of needle insertion, an antegrade direction for both needles was followed.
Fig. 1. 6-year-old fistula with Polish needles inserted for hemodialysis. There was no oozing from the puncture sites. Note that the hubs are at least 2 mm from the skin and the sites from previous needle insertions are clearly visible (modified from Twardowski and Kubara [3]).
An important factor in arteriovenous fistula use and survival is the blood flow through the dialyzer. Higher blood flow also requires bigger needles (gauge 15 or even 14), which are not favorable for fistula complications. In the original study on constant-site needle insertion, blood flow thorough the dialyzer was always 200 ml/min and needles with outer diameters of 1.6 mm (inner diameter of 1.2 mm, gauge 16) were used [2, 3].
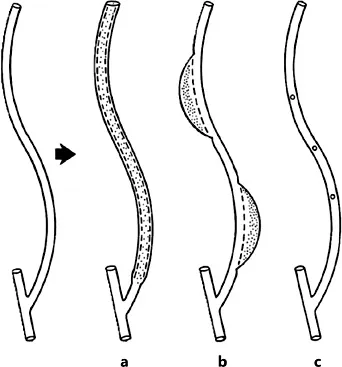
A few years later, Belding Scribner [6, 7] reported his experience with this method in patients with Cimino-Brescia fistulas and confirmed the conclusions of the Twardowski study. In 1984, George Krönung [8] from the University Hospital Bonn (Federal Republic of Germany) presented an analysis of the consequences of repeated fistula punctures and the best technique to avoid fistula damage. Among the three methods (fig. 2), the worst is the area puncture technique, which leads to aneurysms and stenosis. The ‘rope-ladder technique’ is a better technique in which punctures are evenly distributed along the whole fistula length, and the best technique is the repeated puncture of the same site, which he renamed the ‘buttonhole puncture technique’.
After Dr. Twardowski’s departure from Bytom, the constant-site method continued to be used for Maria Zieleniec-Madejska, the first patient in whom the buttonhole method was attempted. She gradually developed various complications, including arteriosclerosis and dialysis-related amyloidosis. When he was in Kraków in 1993, she visited him to ask for some advice. Given her amyloidosis he suggested transplantation, but her candidacy was ultimately rejected because of very poor arteries. Her fistula was lost in 1998, and it was impossible to create another one, so from 1998 she was dialyzed on intravenous catheters. She developed multiple myeloma and passed away in March 2004 after almost 33 years of hemodialysis. She was probably the longest survivor exclusively on dialysis in Poland at that time.
Fig. 2. The three types of puncture localization and their morphologic consequences. a The ropeladder method requires a fistula with long segments suitable for cannulations. b The area-puncture method, where punctures are done in a confined area, weakens the fistula wall and leads to development of (pseudo) aneurysms and strictures. c The buttonhole (constant-site) method is the best and may also be used in fistulas with short segments suitable for sticking [8].
Dr. Twardowski moved to Columbia (Mo., USA) and joined the faculty in the Division of Nephrology, Department of Medicine, University of Missouri, in 1982. Following the success of the constant-site method of needle insertion in Bytom and Lublin, Dr. Twardowski tried to introduce the method after starting his clinical dut...