- Provides clinical examples from the full range of OCD subtypes
- Coverage integrates theory and application
- Decribes case management in detail - from initial assessment to terminating therapy and follow-up
- Shows how IBT can also be generalized and applied to other serious psychiatric disorders
eBook - ePub
Clinician's Handbook for Obsessive Compulsive Disorder
Inference-Based Therapy
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinician's Handbook for Obsessive Compulsive Disorder
Inference-Based Therapy
About this book
This book is the first to bring together new research to offer a hands-on clinical guide to treating people with all types of obsessive compulsive disorder (OCD) using an inference-based therapy (IBT).
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter One
Overview of the IBT Programme
Overview of the IBT Evaluation and Treatment
The present inference-based therapy (IBT) has been developed over the course of the last 15 years utilizing information building upon clinical case studies as well as numerous psychometric, experimental and treatment outcome studies. The approach is a reasoning therapy that focuses on the resolution of the reasons for the initial doubt or obsession responsible for the client's symptoms. The therapy program is highly cognitive in nature often requiring a lot of attention from the therapist in correctly using the model taking fully into account the specific needs of the client. At the same time, there is also a great deal of structure in the current approach, and the accompanying materials are intended to benefit both the therapist and client in their collaborative work.
Step by Step
The idea of the stepped manual is that both client and therapist progress in small steps which simply follow on naturally from each other. The client moves from reflection on a point to intellectual acceptance, to personal and emotional engagement, to enactment. Along the way, metaphors are used to convey the natural nature of the progress and avoid the implication that major leaps out of the ordinary need to be made. In keeping with this ‘natural flow’ metaphor, the therapist should be careful to always locate him or herself and the client on the map of recovery. In particular the conditions to be met before transition from stage to stage are spelt out clearly. We have tried to pinpoint the signs that reveal progress and of course how to deal with no progress.
Broadly speaking, the current stepped programme can be subdivided in three main parts– (1) Education and Foundation, (2) Intervention and (3) Consolidation, each of which consists of a series of different steps. Duration of treatment may vary from client to client, but in most cases, all steps can be provided to the clients in the course of 12 to 20 treatment sessions but number of sessions can be flexible. This allows the therapist to sometimes spend two treatment sessions on one particular step in treatment if the client experiences difficulty, or if further practice reinforcement is necessary before proceeding to the next step.
Each step in treatment includes accompanying worksheets that form the basis for the sessions covering the specific step in treatment. The worksheets are provided to the client after the session to ensure proper integration of the material. In addition, the client is provided with an exercise sheet and a training card as it pertains to each step in treatment. The exercise sheets and training card are intended to ensure the practical application of the material learned during the therapy, and form an essential part of the treatment. In addition, quizzes and cartoons are provided for further consolidation of learning, enhance understanding, and increase the overall complicity of the client and effectiveness of the treatment delivery.
The first part of treatment termed Education and Foundation primarily revolves around education and foundation and lays the foundation for IBT. Step one called When Doubt Begins shows the client how doubt is responsible for most of his or her symptoms. This step is intended to ensure a proper adherence to the model, as well as increase the client's awareness on the origin of his or her symptoms.
The crucial first step is identifying the doubt behind the immediate manifestations of OCD behaviour. The identification then permits establishing the origin and sequence of the obsessional chain ending in the self-sabotage of compulsions and safety behavours. Only later when the everyday doubts are resolved is the underlying self-doubting theme addressed. Why? Because the theme becomes more visible to the client at this point. Self-repositioning towards the authentic ‘real’ self is then easier and more likely to succeed than at the start of therapy. A key exception to this treatment sequence is where the doubting inference may already be close to the self-theme. This may occur in overvalued narrow mono-symptomatic obsession, ‘I could offend the devil’, or in existential ruminations largely centred on the self, ‘I doubt who I am’, or in hoarding, ‘I could be nothing without my objects’. So the self-doubt can be addressed initially or in tandem with immediate obsessional doubts, if it is already visible to the person.
The next step of Education and Foundation termed The Logic behind OCD focuses on the reasoning preceding the doubt and is intended to show the client that the doubt or obsession does not appear out of the blue. Exercises are intended to increase awareness that there is reasoning behind the doubt rather than that the doubt is just ‘happening’ to the person.
The third step of Education and Foundation termed The Obsessional Story expands upon the previous step by showing how obsessional doubt gains its strength and reality value from a convincing narrative leading logically onto the doubt. This is the narrative unit giving credibility to the doubt and will be a primary focus in the course of therapy. The OCD narrative is constructed in collaboration with the client, utilizing the information on reasoning collected so far and filling in any gaps in the story. It is demonstrated to the client how the narrative leads to absorption into the obsession.
Finally, the fourth step of Education and Foundation The Vulnerable-Self Theme locates the OCD within a wider self-theme that makes the person vulnerable to create doubt in specific domains. The self-theme also throws light on the person's type and form of OCD. The vulnerability theme is the self the person fears becoming and is itself yet another OCD story. As noted earlier, the self-theme is derived from the obsessional doubts. This self-theme can be addressed right from the beginning of therapy, especially when the theme already forms a principal doubt in, for example, some ruminative doubts, or the theme can be introduced at a later stage when the person has already overcome doubts leading to more everyday compulsions. All of these four steps of Education and Foundation combine to form the fruitful ground for optimizing effectiveness of subsequent interventions.
The second part of treatment called Intervention attempts to directly change the obsession or doubt. It introduces the central tenet of IBT which is that obsessions are constructed and always occur without any direct evidence. Most crucially, in normal doubt there is always direct evidence or information that supports the doubt. No such direct evidence occurs in obsessional doubt. This concept is introduced from a number of angles in a series of distinct steps eventually resulting in an alternative non-obsessional narrative more in line with reality.
The first step of Intervention termed OCD Is 100% Imaginary establishes with the client that there is no direct evidence in the here and now, and so the OCD story is entirely subjectively generated. The client is shown that the doubt originates 100% from within the person rather than is fuelled from an immediate outside source. The purpose is not yet to invalidate the doubt. The main point to get across is that the doubt originates from the person as opposed to from reality in the here and now.
The second step of Intervention titled OCD is 100% irrelevant takes the point a little further and shows to the client that if the obsessional doubt originates solely from within the person rather than from the outside, then it is 100% irrelevant to the here and now. The crucial point here is that even though the doubt may very well be possible in the abstract, it is still irrelevant ‘now’. Incomplete intellectual adherence to this idea should not prevent the therapist at this point from proceeding to the next step, but may negatively affect the effectiveness of future interventions. However, resolution of the obsessional doubt more likely in subsequent steps if the client intellectually grasps the idea that obsessions are irrelevant.
The third step of Intervention The OCD Bubble helps the client to identify the exact point where he or she crossed over to the imagination and left the world of senses. It is shown to the client that while inside of the OCD Bubble client contact with the physical senses and common sense is lost, and further compulsions only serve to fuel their imagination and rehearse the doubt, and so OCD makes them less secure.
The fourth step of Intervention termed Reality Sensing elaborates on how obsessional doubt is always a false doubt because it goes against reality. Reality sensing is simply trusting and going with the senses rather than doubting and going away from them. An alternative narrative is introduced that takes the senses into account leading to an entirely different conclusion than that which flows from the obsessional doubt. The client is encouraged to begin acting on alternative stories in combination with proper reality sensing. Potential problems with reality sensing are addressed, such as trying to do too much to ‘get into’ reality. The client may experience a void owing to a sense of not doing enough, and is taught how to sense reality without effort.
These four steps of the intervention form the basis for further consolidation of gains made so far in the course of treatment and to boost further progress.
The final part of treatment termed Consolidation attempts to further weaken the obsessional doubt by invaliding the obsessional story, strengthening the alternative story and encouraging the client to act upon this knowledge.
The first step of Consolidation is termed A Different Story where the client is encouraged to elaborate on the non-obsessional story in a natural and practical way. The person develops the art of story telling and how creating and telling stories about events and selves can transport emotions and perceptions and change beliefs.
The second step of Consolidation termed Tricks and Cheats of the OCD Con Artist familiarizes the client with the many tricks and cheats of the OCD that make it seem as if obsessional doubt has something to do with reality. Elements in the obsessional story of the client are addressed as specific devices used by the OCD to generate doubt. This is then followed up with teaching the client specific counter-strategies to trick the OCD con artist.
The third step of consolidation titled The Real Self highlights the selective nature of obsessional doubt as well as the vulnerable self-theme running through the doubt. The client is shown that the selectivity of the obsessional doubt only further invalidates the reality of obsessional doubt. A positive message is transmitted to the client to show that the OCD only affects a specific portion of the client's life, whereas functioning is often healthy in other spheres. Specific exercises are given to the client to strengthen awareness of this selectivity and in knowing the difference between their authentic and OCD selves.
The vulnerable self-theme underlying the OCD is also explored since this theme renders the person vulnerable to doubt in certain areas and not others. This OCD self is also a false self in the same way that the obsessional doubt is false. An important part of overcoming OCD is to find and recognize who the client really is . . . the authentic self. The authentic self, since it is based in reality, is usually the opposite to the OCD self. The authentic self is the self which achieves constructive accomplishments in the world and was always there, albeit masked by the OCD.
The fourth step of consolidation termed Knowing and Doing: Relapse Prevention focuses on the translation of knowledge into action. The client is encouraged to act upon the knowledge that the doubt is false and to identify and correct any thoughts that keep him or her from acting ‘sensibly’. This section addresses the split between knowing how to act and acting on it. Knowing implies behaving. It is not a leap in the dark but a natural progression of the same attitude. Every single thought and belief that still prevent the person from behaving in a noncompulsive way have to be specifically addressed as invalid given the lack of sense of information in the here and now.
Relapse prevention also addresses strategies to maintain gains, foresee difficulties and if necessary strengthen contact with reality with the authentic self and the senses and dispel imaginary doubts.
Finally, a trouble shooting and problem solving section covers technical problems in applying IBT, plus more general or conceptual queries from client and therapist.
Cartoon 1. The doubting dance.

Process Towards Integration
Emphasis is placed within the IBT model on the integration of the model into thought and action, and we illustrate the process by which contact with the IBT model can lead to full integration through a natural progression of accompanying steps.
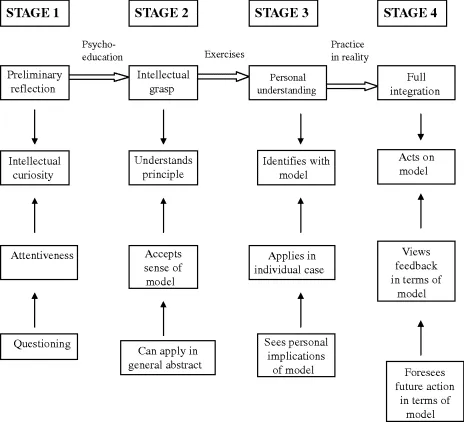
This cognitive schema, inspired by the well-known Prochasky and DiClemente's transtheoretical behavioural model of change, charts the progression from a preliminary reflection on the IBT model through intellectual and personal understanding to a full integration of the model. The therapist acts as guide through the stages combined with interventions designed to prompt insight and advance.
In stage 1, the person needs initially to show an openness and interest in the model. So, for example, psycho-education in the model and its account of aspects of OCD helps move the person along from a preliminary reflection to intellectual grasp. If the person does not show this initial interest, one might question readiness to undertake IBT.
In stage 2, intellectually, the person sees the utility and relevance of the model to OCD and how it can be applied generally. So the person may be able to describe how the model may apply to other people's OCD. In stage 3, in personal understanding the person is comfortable discussing their own obsession in IBT terms. The person begins describing their own symptoms in IBT terms, for example ‘Here I realize I went over the bridge into imagination’, or ‘Yes, this doubt I experienced was definitely obsessional’. Finally, when integrated, the person uses IBT vocabulary to discuss all experiences. The person begins resolving their OCD experiences entirely in IBT terms. ‘I see now how I need to catch the obsession before I cross over the bridge’, ‘I see that OCD was an illusion, making me ima...
Table of contents
- Cover
- Praise for Clinician's Handbook for Obsessive-Compulsive Disorder
- Title Page
- Copyright
- List of Cartoons
- About the Authors
- Acknowledgements
- Introduction
- Chapter One: Overview of the IBT Programme
- Chapter Two: IBT: Evaluation Tools
- Part I: Education and Foundation
- Part II: Intervention
- Part III: Consolidation
- Case Illustrations
- Case Illustrations: Clinical Data
- Answers to Common Queries from Clients
- Therapist Queries
- Quiz Answers Sheet
- Appendix 1: Inferential Confusion Questionnaire (ICQ-EV)
- Appendix 2: IBT Clinical Scales
- Appendix 3: Therapy Evaluation Form and Scale
- Appendix 4: Avoidance and Situational Profile Scale
- Appendix 5: Diary
- Bibliography: Key IBA Publications and Other References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinician's Handbook for Obsessive Compulsive Disorder by Kieron O'Connor,Frederick Aardema in PDF and/or ePUB format, as well as other popular books in Psychology & Clinical Psychology. We have over 1.5 million books available in our catalogue for you to explore.