eBook - ePub
Atlas of Developmental Field Anomalies of the Human Skeleton
A Paleopathology Perspective
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Atlas of Developmental Field Anomalies of the Human Skeleton
A Paleopathology Perspective
About this book
Written by one of the most consulted authorities on the subject, Atlas of Developmental Field Anomalies of the Human Skeleton is the pre-eminent resource for developmental defects of the skeleton. This guide focuses on localized bone structures utilizing the morphogenetic approach that addresses the origins of variability within specific developmental fields during embryonic development. Drawings and photographs make up most of the text, forming a picture atlas with descriptive text for each group of illustrations. Each section and subdivision is accompanied by brief discussions and drawings of morphogenetic development.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
PART I
AXIAL SKELETON
CHAPTER A
SKULL
A-1. CRANIAL VAULT DEVELOPMENT
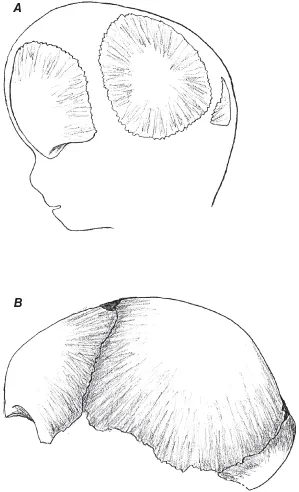
The skull vault arises from the embryonic blastemal (membranous) desmocranium surrounding the developing brain. Neural crest cells are induced by overlying ectodermal tissue to move from the edges of each side of the neural plate folds to form mesenchymal condensations adjacent to specific areas of the developing brain, beginning with the forebrain. Each mesenchymal condensation is associated with a specific part of the brain. By the thirteenth day, these mesenchymal condensations transform into membranous curved plates on each side of the growing brain to form the primordial cranial vault: frontal, parietals, and interparietal squamosa of the occipital bone (Fig. A-1.0). By the seventh week, these bones begin to ossify directly as bony spicules that radiate outward from developing osseous centers within the membranous tissue. The frontal bone ossifies from a pair of osseous centers, one on each side separated by the fetal metopic suture that normally fuses as the two halves grow together after birth by age 2. Each parietal generally ossifies from two osseous centers, one above the other. The squamosal or interparietal portion of the occipital ossifies from a complex of ossification centers with the number varying according to genetic instructions. As the interparietal occipital ossifies, it fuses at the mendosa line with the expanding lower portion of the occipital of the chondocranium as it ossifies from the cartilage.
FIGURE A-1.0. Calvaria development: frontal, parietals, occipital interparietal or squamosa—(A) embryonic membranous bones; (B) newborn bones.
The primitive cranial bones are separated by seams and spaces of connective tissue—sutures and fontanelles. These separations allow the cranial bones to be molded during descent through the birth canal. Postnatal cranial bone growth closes the small fetal sagittal fontanelle before birth. The posterolateral (mastoid) fontanelles close by the end of the first year. The posterior and anterolateral (sphenoid) fontanelles close by 3 months and the anterior fontanelle by 18 months.
CRANIAL VAULT ANOMALIES
A-1.1. Extra Ossicles
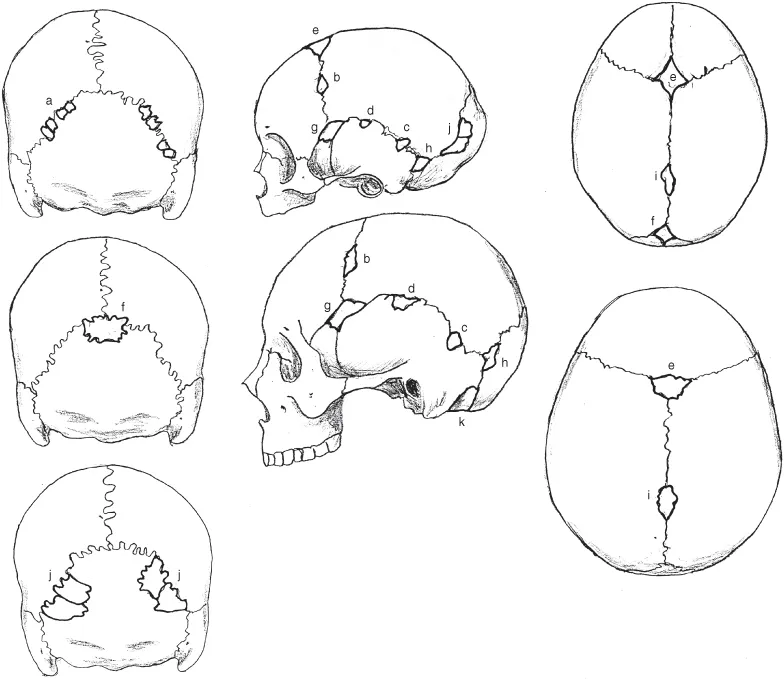
These commonly form within sutures, especially the lambdoidal suture. Less often they develop within the fontanelles (Fig. A-1.1). Multiple and variable extra ossicles (especially along the lambdoidal suture) also occur with cleidocranial dysostosis, a disturbance in the membranous bone tissue development that also affects the membranous development of the clavicle.
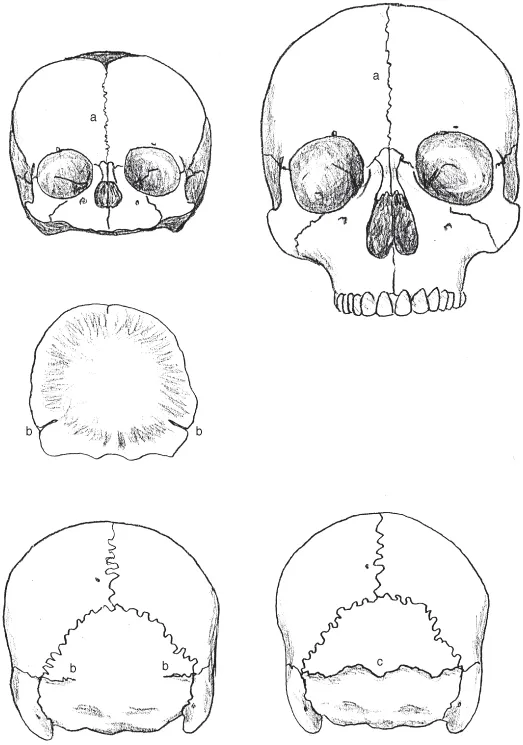
FIGURE A-1.1. Extra ossicles: (newborn and adult) (a) lambdoidal ossicles; (b) coronal ossicles; (c) parietal notch ossicle; (d) temporal squamosa ossicle; (e) bregma (anterior fontanelle) ossicle; (f) lambda (posterior fontanelle) ossicle; (g) epipteric (anteriolateral fontanelle) ossicle; (h) asterion (posterolateral fontanelle) ossicle; (i) obelion (fetal sagittal fontanelle) ossicle; (j) occipital interparietal ossicle; (k) retromastoid ossicle within the chondocranium between the mastoid and occipital.
A-1.2. Extra Sutures
These usually result from the failure of the membranous parts of the same primordial cranial bone to coalesce completely or partially prior to ossification, isolating separate ossification centers within the bone (Fig. A-1.2.1). The metopic suture dividing the infant frontal usually grows together but often remains in place throughout life. The fetal mendosa line between the membranous squamosa and cartilaginous occipital base that normally disappears before birth sometimes remains in place as a complete or incomplete suture. The persistent complete suture gives the appearance of an extra large interparietal occipital bone, commonly referred to as the inca bone (Fig. A-1.2.2).
FIGURE A-1.2.1. Extra parietal sutures: (a) horizontal; (b) vertical (Anderson 1995; Shapiro 1972).
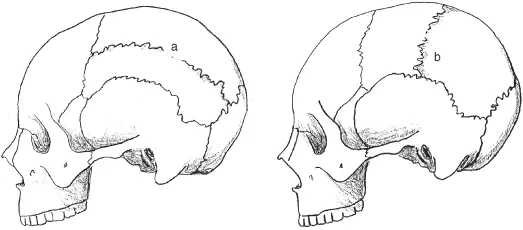
FIGURE A-1.2.2. Extra sutures: (newborn and adult) (a) metopism—retention of infantile suture; (b) remnant fetal mendosa suture; (c) complete retention of fetal mendosa suture (also known as inca bone).
A-1.3. Sutural Agenesis
This is the failure of sutures to develop (completely or partially) between opposing membranous cranial bones. The lack of bony separation can lead to various forms of cranial deformation, especially with more than one type of suture affected (Figs. A-1.3.1–A-1.3.3).
FIGURE A-1.3.1. Sutural agenesis: (A) sagittal suture agenesis—scaphocephalic deformity; (B) coronal suture agenesis—unilateral or partial, may have plagiocephalic deformity, bilateral—brachycephalic form; (C) coronal and lambdoidal suture agenesis—oxycephalic (tower skull) deformity; (D) coronal and sagittal suture agenesis—oxycephalic (tower skull) deformity with bulging occipital; (E) lambdoidal suture agenesis—unilateral or partial, may have plagiocephalic deformity, bilateral—brachycephalic form; (F) lambdoidal and sagittal suture agenesis—dolichocephalic form; (G) metopic suture agenesis—trigonocephalic deformity; (H) temporal squamosa suture agenesis—no deformity; (I) sphenofrontal suture agenesis—no deformity; (J) temporoccipital suture agenesis—no deformity.
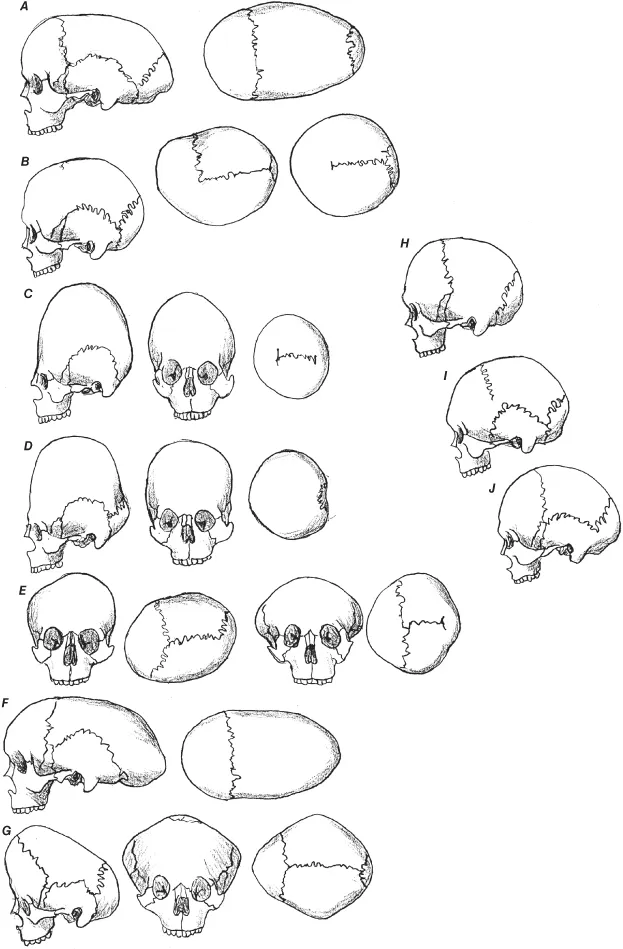
FIGURE A-1.3.2. Sutural agenesis—oxycephaly: coronal and sagittal sutures absent, adult female, Little Colorado River, AZ; (A) lateral and (B) occipital views (Field Museum).
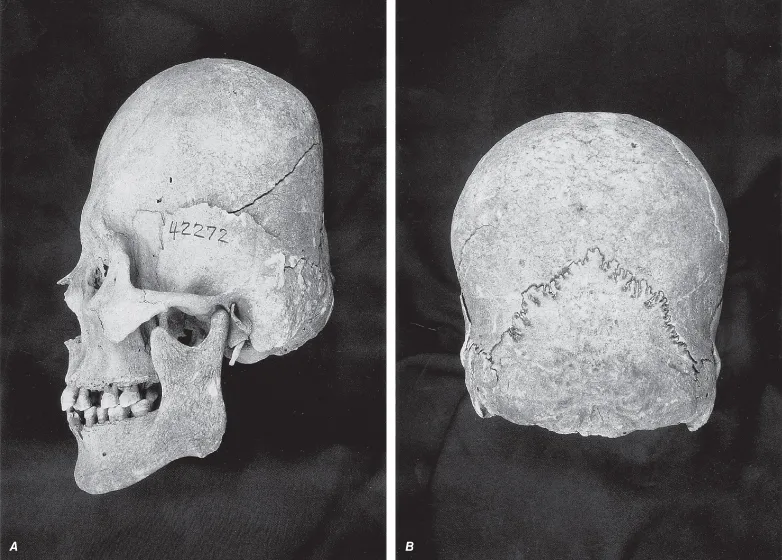
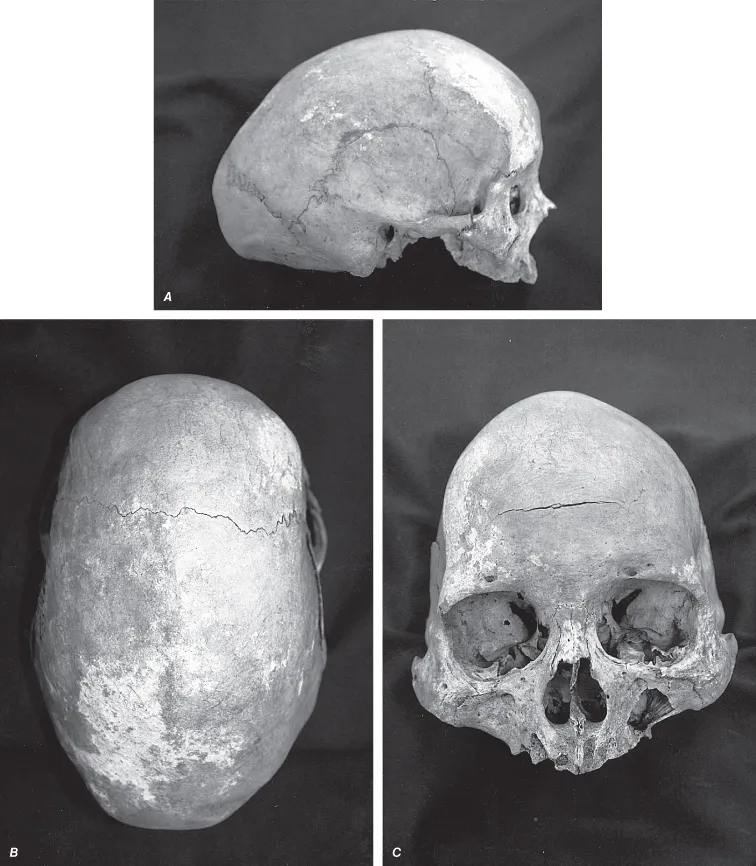
FIGURE A-1.3.3. Sutural agenesis—scaphocephaly: sagittal suture absent, adult male (NMNH 293841), Cerros, Peru; (A) lateral, (B) top, and (C) facial views.
A-1.4. Parietal Thinning
This is the failure of diploe space to develop within the superior–posterior region of the parietal. This creates a somewhat ovoid depression on the surface of the cranium (Fig. A-1.4.1). It has been noticed in children as well as adults. Most often it appears bilateral, but can be seen unilateral, and the affected area is quite thin, becoming more pronounced with age (Fig. A-1.4.2).
FIGURE A-1.4.1. Parietal thinning: (A) bilateral; (B) unilateral.
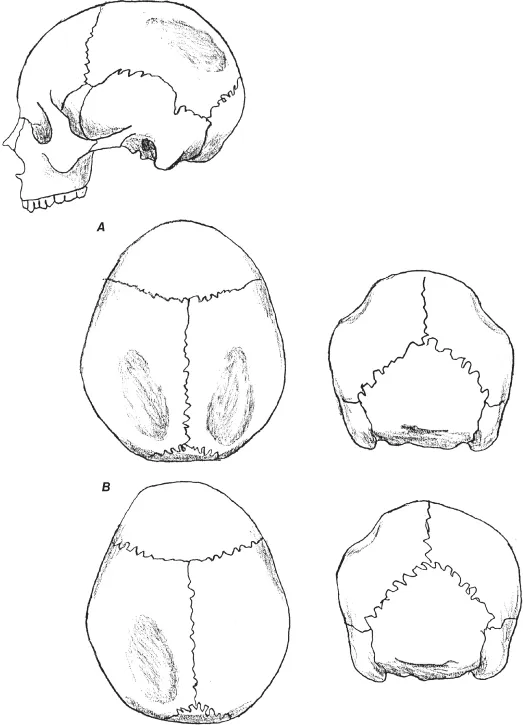
FIGURE A-1.4.2. Parietal thinning close-up: right side, a...
Table of contents
- COVER
- TITLE PAGE
- COPYRIGHT PAGE
- DEDICATION
- PREFACE
- LIST OF FIGURES
- INTRODUCTION
- PART I: AXIAL SKELETON
- PART II: APPENDICULAR SKELETON
- LITERATURE CITED
- INDEX
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Atlas of Developmental Field Anomalies of the Human Skeleton by Ethne Barnes in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Human Anatomy & Physiology. We have over 1.5 million books available in our catalogue for you to explore.