![]()
Part 1 Basics
![]()
Basic science
Introduction
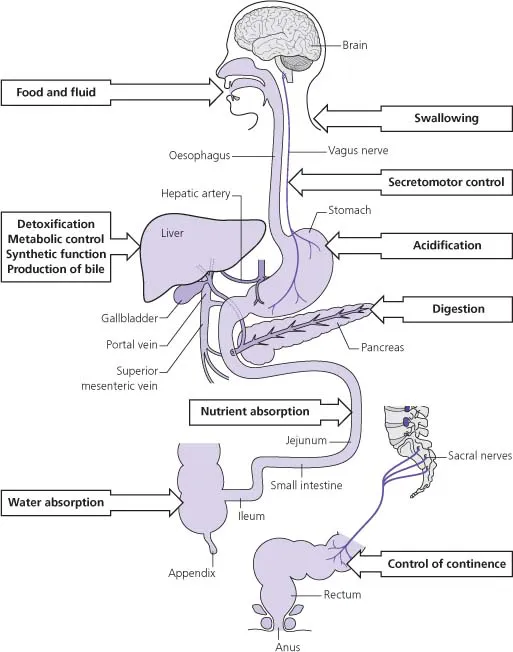
The intestinal tract is essential for maintaining nutrition by appropriate intake of macronutrients, micronutrients, fluid and electrolytes. Intestinal failure can lead to nutritional catastrophe and imbalances in fluid and electrolytes.
The pancreas is the main producer of digestive enzymes that facilitate the extraction of nutrients from food. Pancreatic dysfunction can cause malabsorption of food.
The liver has an essential and central role in metabolism, critical functions in detoxifying and excreting endogenous and exogenous molecules in bile, and in synthesising essential serum proteins such as albumin and clotting factors. Liver failure is rapidly fatal.
Embryology
The entire intestinal tract is derived embryologically from the endoderm, and can be conceptualized as a hollow tube stretching from the mouth to the anus, with the liver and pancreas as gland-like specialised appendages, connected to the main tract by ducts.
Structure
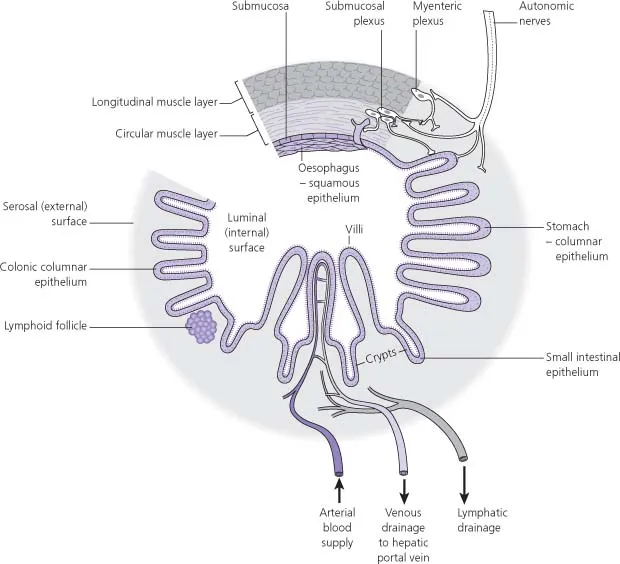
The main intestinal tract has a basic structure that is preserved throughout:
- The innermost layer, facing the hollow lumen, is lined by a specialised layer of epithelial cells that vary from region to region.
- The epithelium is supported by a layer of connective tissue, the lamina propria.
- The lamina propria is surrounded by a layer of smooth muscle, the muscularis mucosae.
- The muscularis is surrounded by the submucosal connective tissue.
- Outside of this are strong layers of muscle, the muscularis propria. This is generally organised in an inner circular layer with fibres running at right angles to the long axis of the tube, and an outer longitudinal layer with fibres running along the long axis.
- The outermost layer of much of the intestinal tract is the visceral peritoneum, which is an epithelial layer.
Most lengths of the small and large intestine are attached to the posterior wall of the abdominal cavity by a length of mesentery, which is comprised of connective tissue covered by a continuation of the visceral peritoneal layer, and through which blood and lymphatic vessels and nerves run.
Blood supply
The arterial blood supply to the intra-abdominal intestinal organs, from stomach to rectum, and including the liver and pancreas, is derived from the coeliac, superior mesenteric and inferior mesenteric arteries, which are direct branches of the abdominal aorta.
The venous drainage of most of the intra-abdominal organs is via the hepatic portal vein, which enters the liver, and provides 75% of the hepatic blood supply. This hepatic portal flow system means that absorbed nutrients first enter the liver, before reaching the systemic circulation.
Nerve supply
Most of the gastrointestinal tract is innervated by the autonomic nervous system with parasympathetic and sympathetic branches. The intestine also contains an intrinsic nervous system organised into interconnected plexuses in the submucosa and the muscularis propria, which is termed the enteric nervous system. This provides isolated segments of intestine with the ability to coordinate secretion and motility without external innervation.
Immune system
The intestinal tract encounters food particles, antigens and potentially harmful microorganisms constantly. Arguably, it must contend with the greatest challenge in defending the organism against infection and other danger, as unlike other areas exposed to the external world, such as the skin and lungs, it also has to make fine distinctions between substances that could be either essential food or lethal foe – ‘salmon or Salmonella?’.
As a consequence, the immune system of the gastrointestinal tract is highly developed and specialised, and contains approximately 70% of all the immune cells in the body.
Anatomy and function
The intestinal tract
Mouth, pharynx and oesophagus
The mouth with teeth, tongue and salivary glands is essential for ingestion of food and nutrition. The senses of taste and smell serve to identify healthy food, and coordinated activity of the muscles of mastication, the tongue and pharynx allow food to be processed and swallowed safely.
The mouth, pharynx and oesophagus are all lined by a stratified squamous epithelium. The muscle layers of the
upper oesophagus are striated skeletal-type muscle, while the muscle layers of the distal oesophagus, like the rest of the intestinal tract, comprise smooth, non-striated fibres.
Stomach
The stomach is J-shaped, wider at the proximal, upper end, known as the body, and narrowing distally to form the antrum, from which the pylorus leads to the duodenum. This shape means that the stomach can act as a reservoir for food after a meal. Strong churning movements of the stomach convert solid food boluses from the oesophagus into slurry called chyme, which passes easily into the duodenum.
The gastric epithelial lining is comprised of a single layer of columnar cells, which is also the case for the rest of the intestinal tract distal to the stomach. In the stomach this epithelial layer is specialised to produce hydrochloric acid from parietal cells, via a specialized K+/H+ transporter, popularly known as the proton pump. This initiates the process of digestion by activating the enzyme pepsinogen, produced by oxyntic cells in the gastric epithelim.
Duodenum
Anatomy
The epithelium of the duodenum is specialised for absorption, comprising a single layer of columnar cells that are lined with microscopic microvilli to increase the surface area for absorption. Furthermore, specialised molecules on the cell surface, including transporters and enzymes, are critically important for this digestive and absorptive function.
The lining of the duodenum, like the rest of the small intestine, is arranged into finger-like projections into the lumen, called villi, which serve to increase the surface area, and indentations into the wall of the intestine, called crypts. The ste...