- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinical Anatomy of the Eye
About this book
Clinical Anatomy of the Eye has proved to be a very popular textbook for ophthalmologists and optometrists in training all over the world. The objective of the book is to provide the reader with the basic knowledge of anatomy necessary to practice ophthalmology. It is recognised that this medical speciality requires a detailed knowledge of the eyeball and the surrounding structures. The specialist's knowledge should include not only gross anatomic features and their development, but also the microscopic anatomy of the eyeball and the ocular appendages. The nerve and blood supply to the orbit, the autonomic innervation of the orbital structures, the visual pathway, and associated visual reflexes should receive great emphasis. The practical application of anatomic facts to ophthalmology has been emphasised throughout this book in the form of Clinical Notes in each chapter. Clinical problems requiring anatomic knowledge for their solution are presented at the end of each chapter. Illustrations are kept simple and overview drawings of the distribution of the cranial and autonomic nerves have been included.
Information
CHAPTER 1
Development of the Eye and the Ocular Appendages
CHAPTER OUTLINE
Introduction
The Eyeball
The Retina
Macular Area and Fovea Centralis
The Optic Nerve
The Lens
The Vascular Lens Capsule
The Lens Capsule
The Ciliary Body and Suspensory Ligaments of the Lens
The Iris
The Anterior and Posterior Chambers
The Vitreous Body
The Cornea
The Sclera
The Choroid
The Extraocular Muscles
Accessory Eye Structures
The Eyelids
The Lacrimal Gland
The Lacrimal Sac and Nasolacrimal Duct
The Orbit
Postnatal Growth
Senile Changes in the Eye
Clinical Notes
Strabismus
Cataract
Glaucoma
Persistent Pupillary Membrane
Coloboma
Absence of Pigment in the Retina and Iris
Cleft Eyelid
Adhesion of Eyelid Margins
Atresia of the Nasolacrimal Duct
Congenital Fistulas of the Lacrimal Sac
Clinical Problems
Answers to Clinical Problems
Introduction
The eye is formed from both ectoderm and mesenchyme. The ectoderm that is derived from the neural tube gives rise to the retina, the nerve fibers of the optic nerve, and the smooth muscle of the iris. The surface ectoderm on the side of the head forms the corneal and conjunctival epithelium, the lens, and the lacrimal and tarsal glands. The mesenchyme forms the corneal stroma, the sclera, the choroid, the iris, the ciliary musculature, part of the vitreous body, and the cells lining the anterior chamber. The endothelium of the cornea is believed to be of neural crest origin.
The reader should note the importance of the induction of one ocular tissue by another during development. The lens, for example, is induced to develop by the presence of the optic vesicle. The presence of the developing lens induces the formation of the cornea and stimulates the development of the vitreous body. The presence of the developing lens is also important for the normal growth of the pigment layer of the retina, which in turn influences the differentiation of the mesenchyme into the choroid and the sclera. How this induction process is brought about remains to be determined.
The Eyeball
The rudimentary eyeball develops as an ectodermal diverticulum from the lateral aspect of the forebrain (Fig. 1-1). The diverticulum grows out laterally toward the side of the head, and the end becomes slightly dilated to form the optic vesicle, while the proximal portion becomes constricted to form the optic stalk (Fig. 1-1). At the same time, a small area of surface ectoderm overlying the optic vesicle thickens to form the lens placode. The lens placode invaginates and sinks below the surface ectoderm to become the lens vesicle. Meanwhile, the optic vesicle becomes invaginated to form the double-layered optic cup. The inferior edge of the optic cup is deficient, and this notch is continuous with a groove on the inferior aspect of the optic stalk called the optic or choroidal fissure (Fig. 1-1). Vascular mesenchyme now grows into the optic fissure and takes with it the hyaloid artery. Later, this fissure becomes narrowed by growth of its margins around the artery, and by the seventh week of embryonic development the fissure closes, forming a narrow tube, the optic canal, inside the optic stalk (Fig. 1-2). Failure of the fissure to close completely results in coloboma formation (see p. 18), which may include the pupil, ciliary body, and choroid or optic nerve. By the fifth week, the lens vesicle loses contact with the surface ectoderm and lies within the mouth of the optic cup, the edges of which form the future pupil (Fig. 1-3).
The Retina
The retina develops from the optic cup. For purposes of description, the retina may be divided into two developmental layers, the pigment layer and the neural layer.
The pigment layer is formed from the outer thinner layer of the optic cup (Fig. 1-3). It is a single layer of cells that become columnar in shape and develop pigment granules (melanosomes) within their cytoplasm.
Figure 1-1
(A) Dorsal view, showing the formation of the optic vesicle, which grows out as a diverticulum from the lateral aspect of the forebrain. (B) Coronal section of diencephalon, showing a thickening of the surface ectoderm overlying the optic vesicle to form the lens placode. (C) Coronal section of diencephalon, showing the lens placode invaginating and sinking below the surface ectoderm. Note that the optic vesicle is also becoming invaginated. (D) The formation of the lens vesicle, the optic cup, and the choroidal fissure.
(A) Dorsal view, showing the formation of the optic vesicle, which grows out as a diverticulum from the lateral aspect of the forebrain. (B) Coronal section of diencephalon, showing a thickening of the surface ectoderm overlying the optic vesicle to form the lens placode. (C) Coronal section of diencephalon, showing the lens placode invaginating and sinking below the surface ectoderm. Note that the optic vesicle is also becoming invaginated. (D) The formation of the lens vesicle, the optic cup, and the choroidal fissure.
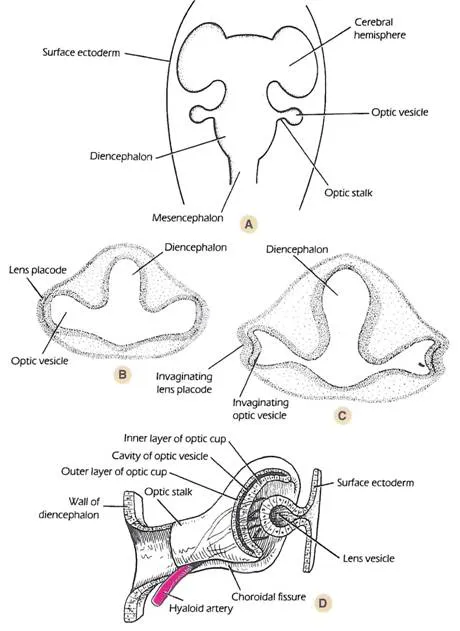
Figure 1-2
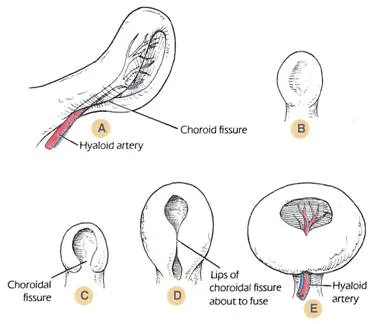
(A-E) A series of diagrams illustrating the formation of the optic cup from the optic vesicle. Note that the inferior edge of the optic cup is deficient, and that this notch is continuous with the choroidal fissure. The lips of the choroidal fissure fuse around the hyaloid artery and vein.
(A-E) A series of diagrams illustrating the formation of the optic cup from the optic vesicle. Note that the inferior edge of the optic cup is deficient, and that this notch is continuous with the choroidal fissure. The lips of the choroidal fissure fuse around the hyaloid artery and vein.
The neural layer is formed from the inner layer of the optic cup. However, in the region of the cup that overlaps the lens, the inner layer is not differentiated into nervous tissue. This anterior one-fifth of the inner layer persists as a layer of columnar cells, which, together with the pigmented epithelium of the outer layer, extend forward onto the posterior surface of the developing ciliary body and iris (Fig. 1-4).
The posterior four-fifths of the inner layer of the optic cup undergoes cellular proliferation, forming an outer nuclear zone and an inner marginal zone, devoid of nuclei (Fig. 1-3). Later, the cells of the nuclear zone invade the marginal zone so that the neural part of the retina is made up of an inner and an outer neuro-blastic layer. The inner neuroblastic layer forms the ganglion cells, the amacrine cells, and the bodies of the sustentacular fibers of Müllre. The outer neuroblastic layer gives rise to the horizontal and rod and cone bipolar nerve cells and the rod and cone cells. By the eighth month of fetal life all the layers of the retina can be recognized. It should be noted that the retinal photoreceptor cells continue to form after birth so that the retina develops the ability for increasing resolution and sensitivity.
Thus, the inner layer of the optic cup may be divided into a small non-nervous portion near the edge of the cup and a large photosensitive portion, the two being separated by a wavy line, the ora serrata (Fig. 1-4).
It is interesting to remember that the cavity of the optic vesicle is continuous through the optic canal with the cavity of the diencephalon (i.e., that part which will form the third ventricle). Early in development, the outermost layer of cells of the nuclear zone have cilia, which are continuous with the ciliated ependymal cells of the third ventricle. Later, during the seventh week of development, the cilia of the cells of the nuclear zone disappear and are believed to be replaced by the outer segments of the rods and cones during the fourth month.
Figure 1-3
The eye at different stages of development. (A) The formation of the lens from the lens vesicle and its nourishment by the hyaloid artery. Note the further development of the inner and outer layers of the optic cup and the continued presence of the cavity of the optic vesicle. (B) The development of the cornea, the anterior chamber, and the pupillary membrane. The cavity of the lens vesicle is still present. The eyelids have fused and remain so until the seventh month before birth.
The eye at different stages of development. (A) The formation of the lens from the lens vesicle and its nourishment by the hyaloid artery. Note the further development of the inner and outer layers of the optic cup and the continued presence of the cavity of the optic vesicle. (B) The development of the cornea, the anterior chamber, and the pupillary membrane. The cavity of the lens vesicle is still present. The eyelids have fused and remain so until the seventh month before birth.
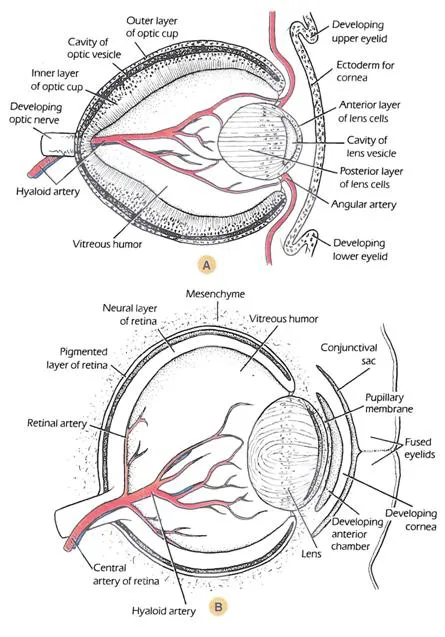
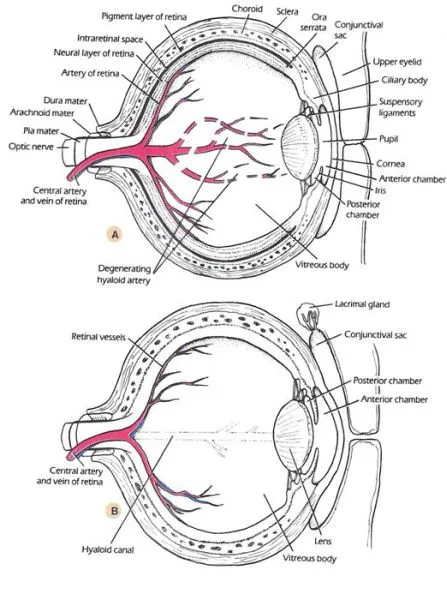
Figure 1-4
(A, B) The eye in advanced stages of development. Note the degeneration of the hyaloid vessels and the persistence of the hyaloid canal in the vitreous body. The remains of the hyaloid vessels become the central artery and vein of the retina. The lacrimal gland has developed as an outgrowth of the conjunctival sac.
(A, B) The eye in advanced stages of development. Note the degeneration of the hyaloid vessels and the persistence of the hyaloid canal in the vitreous body. The remains of the hyaloid vessels become the central artery and vein of the retina. The lacrimal gland has developed as an outgrowth of the conjunctival sac.
Macular Area and Fovea Centralis
The macular area first develops as a localized increase of superimposed nuclei in the ganglion cell layer, lateral to the optic disc, just after midterm. During the seventh month there is a peripheral displacement of the ganglion cells, leaving a central shallow depression, the fovea centralis. The inner segments of the foveal cones decrease in width, but the outer segments are elongated. This permits an increase in foveal cone density. At birth, the ganglion cells have been reduced to a single layer in the fovea, and by 4 months of age the cone nuclei in the center of the fovea have no ganglion cells covering them. The reason for the newborn’s imperfect central fixation is that the cones do not fully develop until several months after birth.
The Optic Nerve
The ganglion cells of the retina develop axons that converge to a point where the optic stalk leaves the posterior surface of the optic cup. This site will later become the optic disc. The axons now pass among the cells that form the inner layer of the stalk (Fig. 1-5). Gradually, the inner layer encroaches on the cavity of the stalk until the inner and outer layers fuse. The cells of the optic stalk form neuroglial supporting cells to the axons, and the cavity of the stalk disappears. The stalk, together with the optic axons, forms the optic nerve. The axons of the optic nerve begin to develop their myelin sheaths just before birth, but the process of myelination continues for some time after birth. The partial decussation of the axons of the two optic nerves forms the optic chiasma. The hyaloid artery and vein become the central artery and vein of the retina.
The optic nerve axons leave the optic chiasma and grow backward as the optic tracts and the majority pass to the lateral geniculate body and to the tectum of the midbrain.
The Lens
The rudimentary lens is first seen as a thickening of the surface ectoderm, the lens placode, at 22 days’ gestation; it overlies the optic vesicle (Fig. 1-1). The lens placode invaginates and sinks below the surface ectoderm to form the lens vesicle, which consists of a single layer of cells covered by a basal lamina.
The cells forming the posterior wall of the lens now rapidly elongate and become filled with proteins called crystallins, which make them transparent (Figs. 1-3 and 1-4). These densely packed elongated cells are known as the primary lens fibers. The base of each elongating cell remains attached to the basal lamina posteriorly while their apices grow forward toward the anterior lens epithelium so that the cavity of the lens vesicle gradually becomes obliterated. The lengthening of the cells first occurs at the center of the posterior wall, which projects forward into the lens cavity. The nuclei of the lens fibers move anteriorly within the cells to form a line convex forward called the nuclear bow (Fig. 1-6). The primary lens fibers now become attached to the apical surface of the anterior lens epithelium and their nuclei disappear.
Figure 1-5
A series of diagrams showing the formation of the optic nerve from the optic stalk, as seen in cross-section. (A) The cavity of the optic stalk. (B) The choroidal fissure occupied by the hyaloid vessels, which become the central artery and vein of the reti...
A series of diagrams showing the formation of the optic nerve from the optic stalk, as seen in cross-section. (A) The cavity of the optic stalk. (B) The choroidal fissure occupied by the hyaloid vessels, which become the central artery and vein of the reti...
Table of contents
- Cover
- Contents
- Title
- Copyright
- Preface
- CHAPTER 1: Development of the Eye and the Ocular Appendages
- CHAPTER 2: An Overview of the Anatomy of the Skull
- CHAPTER 3: The Orbital Cavity
- CHAPTER 4: The Paranasal Sinuses
- CHAPTER 5: The Ocular Appendages
- CHAPTER 6: The Eyeball
- CHAPTER 7: The Anatomy of the Eyeball as Seen with the Ophthalmoscope, Slit Lamp, and Gonioscope
- CHAPTER 8: Movements of the Eyeball and the Extraocular Muscles
- CHAPTER 9: The Orbital Blood Vessels
- CHAPTER 10: Cranial Nerves—Part I: Those Nerves Directly Associated with the Eye and Orbit
- CHAPTER 11: Cranial Nerves—Part II: The Nerves Not Directly Associated with the Eye and Orbit
- CHAPTER 12: The Autonomic Nervous System
- CHAPTER 13: The Visual Pathway
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Anatomy of the Eye by Richard S. Snell,Michael A. Lemp in PDF and/or ePUB format, as well as other popular books in Medicine & Opthalmology & Optometry. We have over 1.5 million books available in our catalogue for you to explore.