![]()
1
Organ Retrieval Logistics
Murat Akyol1 and Victor L. Tswen Wen2
1Royal Infirmary of Edinburgh; College of Medicine and Veterinary Medicine, University of Edinburgh, UK
2Division of Hepatobiliary and Pancreatic Surgery, Liver Transplant Programme, Department of Surgery, National University Hospital; Nanyang Technological University, Singapore
Introduction
There are very few countries where organ donation is not covered by the provisions of law or is expressly prohibited. However, healthcare infrastructure or cultural and religious traditions have prevented widespread adoption of the practice in many societies. Substantial differences exist in donation rates even amongst countries of similar socio-economic status, sharing a similar cultural and religious heritage and similar legislative framework. Such differences testify to the important role of logistics in the success of organ transplantation.
Organ transplantation involves two surgical procedures: the retrieval of an organ from a donor and implantation of the organ to a recipient.
This chapter specifically deals with logistical issues surrounding organ retrieval. The details of the surgical procedures required to retrieve organs are covered in subsequent chapters of the book. The logistical issues discussed refer to organ retrieval from deceased donors only.
Diagnosis of death – DBD and DCD donation
It is acknowledged worldwide that the irreversible loss of the capacity for consciousness combined with the irreversible loss of the capacity to breathe equates to death. Irreversible loss of brainstem functions produces this state. Therefore demonstration that the functions of the brainstem have irreversibly ceased allows diagnosis of death.
On the background of this principle, different legal definitions of death have evolved in different countries.
Donation after brain death (DBD)
In the UK demonstration of the absence of all the functions of the brainstem by clinical tests is adequate for the diagnosis of brainstem death (BSD) to be made, providing that severe metabolic disturbance and potential effect of drugs and hypothermia have been excluded and a cause has been established. Other countries require additional criteria such as demonstration of lack of electrical activity in EEG or demonstration of the absence of blood flow to the brain by imaging. Criteria used to diagnose BSD in children are the same as those in adults, but it should be noted that the diagnosis of BSD in infants under the age of 2 months is not appropriate or possible.
In order to test for BSD, the patient must be in an unresponsive coma, having sustained ‘irreversible’ brain damage of known aetiology.
Potential reversible circulatory metabolic and endocrine disturbances must have been ruled out as the cause of continuation of unconsciousness:
- Drugs: sedative, muscle relaxants
- Hypothermia < 35°C
- Circulatory, metabolic, endocrine disturbance
In DBD donors, circulation and the oxygenation of peripheral tissues are maintained after death. This allows better preservation of function in the organs to be retrieved and transplanted. The range of organs suitable for transplantation is greater in DBD donation and in general the outcome of transplantation using DBD donor organs is better.
BSD testing:
- Absence of pupillary response to light (occulomotor III cranial nerve)
- Absence of corneal reflexes (trigeminal V cranial nerve)
- Absence of caloric responses
- No motor response in the distribution of the cranial nerves (trigeminal V sensory supply to upper face and facial VII cranial nerves)
- No cough or gag reflex (glossopharyngeal IX and vagus X cranial nerves)
- Testing for apnoea
Death following cessation of cardiorespiratory function – DCD donation
Death can also be diagnosed by an appropriately qualified individual, by confirming irreversible cessation of cardiac, respiratory and neurological activity. In practice the irreversibility of the loss of neurological function is inferred from the length of time that breathing and circulation has been absent.
The cessation of cardiac activity can be determined by the absence of pulses and heart sounds. In the hospital setting, demonstration of asystole on ECG or the absence of blood flow in direct arterial pressure monitoring may also supplement the diagnosis. After 5 minutes of continued absence of circulation and absence of breathing, the absence of pupillary or corneal reflex is tested to confirm cessation of neurological function also. This category of deceased organ donation (previously also referred to as non-heart beating donors – NHBD) is called donation after cardiac death or donation after circulatory death (DCD).
Organ donors in this category are patients who have often sustained catastrophic irrecoverable brain injury and in whom further treatment has been considered futile.
Any decision about futility of further treatment and whether or not active treatment should be withdrawn must be made only in the interest of the patient and with no regard to any consideration of potential organ donation.
When the doctors caring for the patient have made the decision that further treatment is futile, the timing of the withdrawal of treatment can be coordinated, to allow for organ retrieval to take place after circulatory death is diagnosed.
In the early days of organ transplantation, prior to the establishment of criteria to diagnose BSD, this type of donation was the only means to provide organs for transplantation from deceased donors. In the last 10 years there has been a revival of the concept and the practice of DCD. DCD donors provide a variable but increasing proportion of the deceased donor organs transplanted. Specific considerations about retrieval of organs from DCD donors and transplantation of such organs are dealt with in the relevant chapters of this book.
It should be noted that the practice of donation after circulatory death is expressly forbidden by law in certain countries, notably in Germany.
Evolution of organ donation and the legal framework governing organ donation
Historically, even after donation after brain death became accepted practice, the responsibility for retrieving organs from deceased donors rested with the surgical teams of individual transplant units. The multiorgan retrieval procedure involved separate teams from kidney, liver, pancreas and cardiothoracic transplant units to travel to and assemble at the donor hospital.
As organ transplantation became established practice and activity levels increased, it became evident that better coordination of organ retrieval from multiorgan donors and regulation of the allocation of organs for transplantation were required. The differences in statute and social–cultural norms in different countries naturally resulted in varying forms of regulation of organ donation. Broadly speaking the laws dealing with authority for organ retrieval can be divided into two categories:
1 opting out systems where it is assumed that the deceased had no objection to donation unless such objection had been expressly registered prior to death, and
2 opting in systems where prior consent is not assumed and some indication or evidence is required that donation was the wish of the deceased or donation requires consent from relatives.
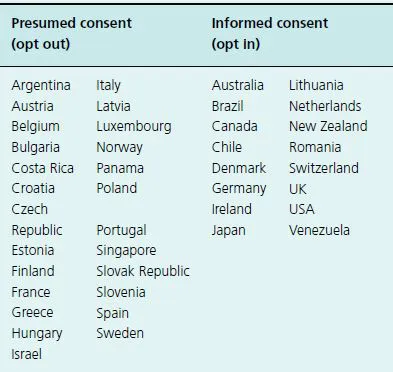
Table 1.1 Donor legislation in various countries.
The legal requirements for donation vary across the globe (Table 1.1) [1,2]. In some countries, an opt-in law, which requires informed consent from the relatives prior to proceeding to donation, is in place. Most European countries have adopted the opt-out or presumed consent law, whereby organs are removed from every identified donor unless they have expressed their wishes against donation (‘hard form’ opt out) or after inquiring from the relatives whether they were aware of such wishes (‘soft form’ opt out).
There is some evidence that the introduction of a decentralized organ procurement system has led to an increase in the number of organ donors [3,4]. It is yet unclear whether replacing an ‘informed consent’ with ‘presumed consent’ legislation has a similar effect on organ donation rates, but some studies [5,6] suggest that a significant increase was noted in countries where the change in legislation was adopted.
Organ retrieval teams and organ transplantation units
Many countries worldwide have gradually moved to a varying degree of separation of the multiorgan retrieval process from the process of organ transplantation. Whilst the details of organ retrieval services vary around the world, there is broad agreement about the principles and standards that apply to successful retrieval of organs from deceased donors.
The key to successful organ retrieval is cooperation between the three essential components, namely donor coordinators, the organ retrieval team and the transplant units.
Donor coordinators
Donor coordinators may be affiliated to transplant centres or be part of an independent organization. Transplant coordinators who remain affiliated to transplant units and serve a dual role as donor and recipient coordinators may fulfill each role equally effectively and this model may arguably have some benefits. However, in terms of one of the most important outcome measures, namely maximizing the potential from deceased donation, international experience and the balance of evidence suggests that dedicated donor coordinators based in potential donor hospitals is a superior model [7].
A wide network of donor coordinators based in local hospitals is the key component of a successful organ donation programme.
In some of the countries with the highest deceased donation rates such as Spain, Portugal and Italy, there are donor coordinators based in every hospital in the country. They play an important role in raising and maintaining the awareness of donation and provide education and support to staff of potential donor hospitals. In the case of DBD donation, donor coordinators will often help approach the donor family, take part in the process of consent or authorization for donation, provide help with donor management in the critical care unit and support the donor family during the process of donation. When required, donor coordinators will a...