![]()
Part 1
The Rhythms
![]()
Normal Sinus Rhythm
DESCRIPTION
This, technically, isn't an arrhythmia at all, but needs to be included simply because it's very important to be able to call something “normal” if it really is!
The key is that it's regular, that it's between a rate of 60 and 100, and most importantly, that every QRS is preceded by a P wave at the proper interval. The complexes may be wide or narrow, but they must have a preceding P wave.
The rhythm is regular, nice P waves, not too fast, not too slow, and as Dr. Goldilocks1 would say, “Just right!”
HABITAT
This rhythm may be found anywhere, and actually may be seen inhabiting most cardiac monitors, which might make one wonder why that patient is being monitored in the first place. It usually means the patient is in some kind of equilibrium with the world: not too hot, not frightened, not in pain, not suffering from bad heart failure, breathing comfortably … in short, at least by the monitor, doing all right.
CALL
“Can I take this patient off telemetry?”
RESEMBLANCE TO OTHER ARRHYTHMIAS
It's regular, so it could be confused with any other rhythm that's regular, but the key is that there's a P wave in front of every QRS and the rate is 60–100. A junctional rhythm is regular but has no P waves.
CARE AND FEEDING
Just keep up what you're doing! We don't want to speed things up or slow things down. So avoid excitement, avoid pain, don't burn your tongue on hot coffee – in short, just do what your mother told you to do.
1 Dr. Goldilocks was a famous electrophysiologist at New York University in the late 1980s.
![]()
Preexcitation
DESCRIPTION
Technically this isn't an arrhythmia (actually, even non-technically it isn't!) but this condition provides the substrate for some crazy arrhythmias, so I thought I'd include it. Your attendings always like to throw this ECG at you, so if you can recognize preexcitation you will definitely impress them.
Preexcitation is to the electrophysiologist as foreplay is to married couples. Let's face it, those studies are long and keep those electrophysiology guys in the lab all night!
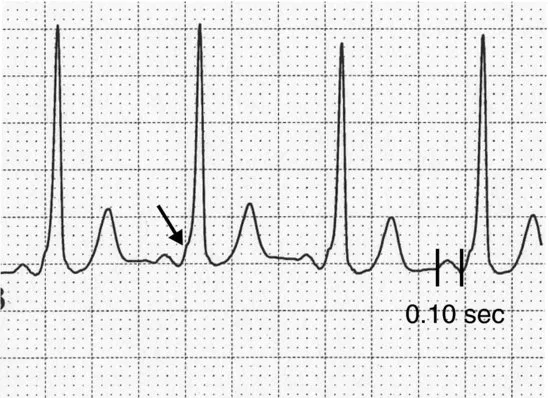
Actually, this is a situation where there is an extra, or accessory, electrical connection between the atrium and ventricle, which can provide a quicker route than the atrioventricular (AV) node for electricity to travel between the two chambers. Creative physiologists named these accessory pathways accessory pathways, which are strands of muscle that are congenitally present and “bridge” the fibrous tissue that electrically insulates the atria from the ventricles. These pathways can conduct electricity and often manifest themselves on the surface ECG by producing a characteristic short PR (because the impulse skips the AV node) and a wide QRS (because the initial part of ventricular activation is via the accessory pathway which activates the ventricle separately from its normal conduction system). The latter part of the ventricular complex, however, is narrow, as the impulse that is working its way through the AV node finally flashes down the normal conduction system. The QRS has a hump at its onset, called a delta wave (see arrow), not to be confused with the faucet or the force.
In sinus rhythm, unless someone looked at the ECG, no one would know preexcitation was present. In sinus rhythm preexcitation is completely asymptomatic. However, these dual pathways can make for some funky arrhythmias: an impulse can travel down the accessory pathway and up the AV node (or the other way around), creating a small, rapidly conducting circuit which can cause an impressive tachycardia. These would look for all the world, depending on the direction the arrhythmia took, like a supraventricular tachycardia or a ventricular tachycardia. Worse yet, patients with preexcitation are prone to developing atrial fibrillation which can be particularly rapid since the accessory pathway may not slow the impulses the way the normal AV node does.
HABITAT
These can be found anywhere, but most are found accidentally when somebody has an ECG done for another reason.
CALL
“Is Wolff–Parkinson–White a sausage company or a law firm?”
RESEMBLANCE TO OTHER ARRHYTHMIAS
In sinus rhythm, preexcitation can be confused with sinus rhythm with a bundle branch block. With preexcitation, the key is the short PR and the delta wave, with the terminal part of the QRS being narrow. During a tachycardia all bets are off; in atrial fibrillation your only clue to the presence of preexcitation may be that it is particularly rapid, with a mix of narrow and wide beats, depending on which pathway conducts the impulse. During other tachycardias it may be very hard to tell if there is underlying preexcitation.
CARE AND FEEDING
If the patient is in sinus rhythm, you don't have to do anything except maybe make an appointment for him or her to see an electrophysiologist, since some of these patients are actually at risk for sudden death from their rhythm disturbances, especially rapid atrial fibrillation. If the patient is known to have preexcitation and is actually in a tachycardia, especially atrial fibrillation, like Siberian tigers or polar bears it is best left to the experts to care for. Many of the responses to pharmacology are paradoxic; if there was an emergency and the patient was unstable, probably the safest thing to do is just to cardiovert the rhythm back to sinus rhythm without getting sucked into the murk of odd drug reactions.
![]()
Sinus Bradycardia
DESCRIPTION
Just like sinus rhythm, but slower; it is defined as sinus rhythm (every QRS preceded by a proper P wave) with a rate under 60.
HABITAT
Boring lectures, a Kenny G concert, inferior infarcts, sleep apnea, or too much β-blocker.
CALL
“Why is everyone running into in my room and looking at me?”
RESEMBLANCE TO OTHER ARRHYTHMIAS
This looks like sinus rhythm, only slower. When it's really slow (rates into the 30s) you might think it's a junctional rhythm, but the presence of P waves with the proper PR interval would indicate it's definitely a sinus rhythm.
CARE AND FEEDING
Probably here more than anywhere else, it's a question of “when in doubt, check the patient”! If the heart rate is 30 but the patient is fine, don't do anything. If the heart rate is slow and the patient is dizzy or hypotensive, then intervene. Here a little atropine might help in the short term. Often withdrawal or reducing the dose of “slower-downers” (such as β-blockers, diltiazem, digoxin, verapamil, or some antiarrhythmics) over time would allow the heart rate to increase. Shouting or showing the patient his or her bill might help also, but if the heart rate stays low and the patient is symptomatic, a pacemaker might be in order.
![]()
Sinus Tachycardia
DESCRIPTION
The same as sinus rhythm, only faster: by definition, sinus rhythm with a rate over 100. Each QRS is preceded by a proper P wave. If you are seeing rates over 140 in a patient resting in bed, either they're REALLY sick or it may not be a sinus tachycardia at all (i.e., some sort of supraventricular tachycardia in disguise, see below). On the other hand, if the patient is running on a treadmill or pursued by a carnivore, a sinus tachycardia at 160 may be quite appropriate.
HABITAT
Commonly found where people are frightened, stressed, hurt, or in pain, such as in an Emergency Department or Operating Room, or if you are a medical student presenting a case to the Chief of Service or taking a final exam. The rhythm is often driven by adrenaline, which is why it is never found during mandatory infection control handwashing updates. But you may commonly see this with fevers, trouble breathing, pain, blood loss, or dehydration – anything that fires up the “fight or flight” system and gets the adrenaline pumping. Some medications themselves can speed up the heart rate, like bronchodilators or dopamine. Don't forget that accidentally omitting someone's β-blocker can result in fantastic sinus tachyca...