![]()
1 Patient Signalment and History
Louise L. Southwood
Department of Clinical Studies, New Bolton Center, School of Veterinary Medicine, University of Pennsylvania, Kennett Square, PA, USA
Chapter Outline
Importance of the patient’s history
Signalment
Obtaining the patient’s history
Initial historySpecific signs
Duration of colic signs
Reproductive status of mares
Obtaining a more detailed historyAppetite, water consumption, defecation, and urination
ManagementFeeding regimen
Water source
Exercise regimen, pasture access, and housing
Recent transportation
Geographical areas in which the horse has been housed
Gastrointestinal parasite control
Vaccination
Medical historyPrevious colic and colic surgery
Other medical problems and current medication
Medical problems of other horses
Crib biting or windsucking
Application of the patient’s history
Importance of the patient’s history
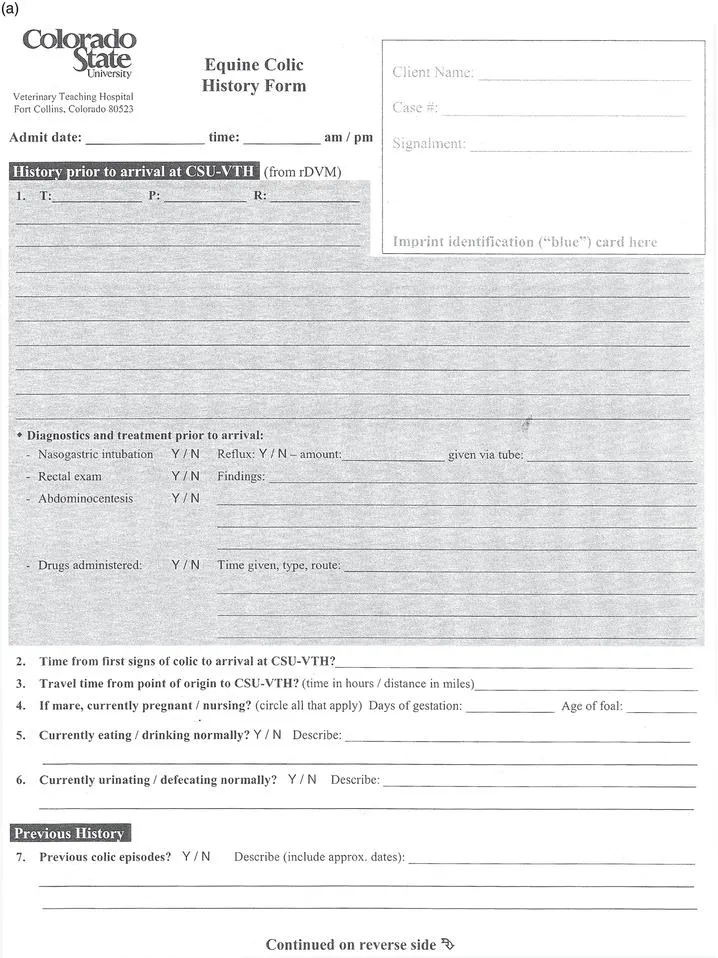
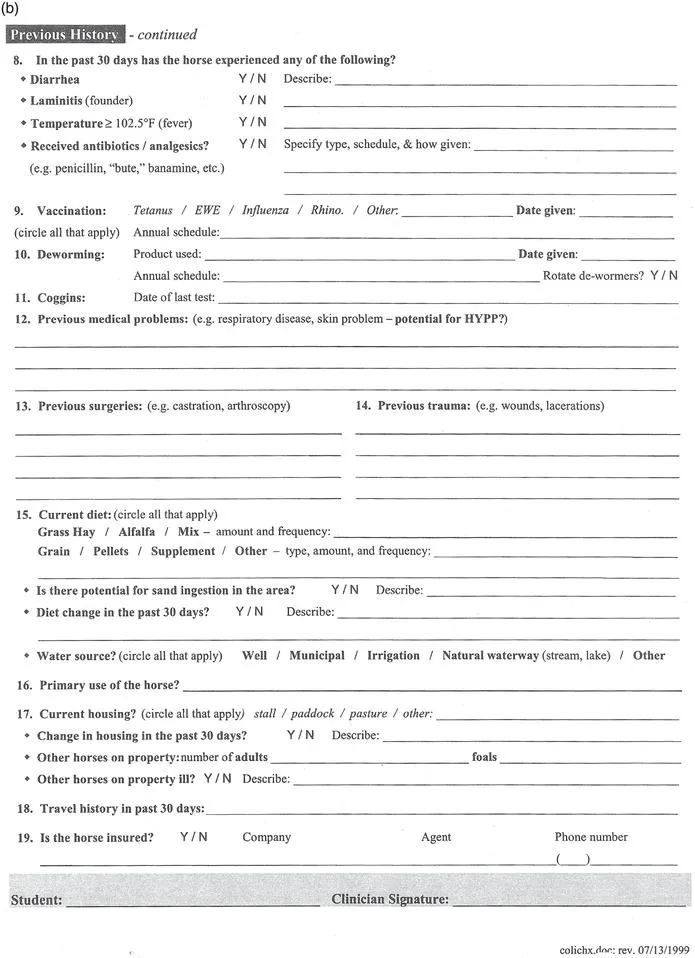
Obtaining a detailed history provides information that can be used to formulate a differential diagnosis list for the horse with colic, direct treatment, and devise a colic prevention plan. Having a standardized history sheet (Figure 1.1) as part of the medical record will streamline the history-taking procedure and ensure details are not omitted. Recording the history as part of the medical record is also important to provide accurate information for referral, for reference in the case of future colic episodes, and as part of a preventative medicine program.
Signalment
Knowledge of the patient’s signalment, namely, age, breed, and gender, is extremely important during evaluation for colic. While gas colic is by far the most common diagnosis across most age, breed, and gender categories,28 the signalment is critical for forming a differential diagnoses list. Gas colic can be defined clinically by horses with mild to moderate pain that resolves spontaneously or with a single dose of an analgesic drug and accounts for about 70–80% of colic episodes.28 Typical differential diagnoses for equine patients of various signalments are shown in Table 1.1.
Signalment is also important because it may direct the history-taking process. For example, (1) if you are presented with a mare showing colic signs, the reproduction status requires investigation; (2) if you have an older horse, underlying diseases should be considered; and (3) in the case of a neonate, questions pertaining to parturition, passive transfer of maternal antibodies, and clinical signs shown by other foals on the farm should be asked. Specific questions are addressed below.
Table 1.1 Differential diagnoses other than gas colic for patients of a specific signalment.
|
| Neonate (p. 279) | - Meconium retention (p. 222, 279)
- Enterocolitis (p. 215, 279)
- Hypoxic-ischemic syndrome (p. 279)
- Jejunal intussusceptions (p. 213, 280)
- Jejunal volvulus (p. 212, 280)
- Atresia coli or jejuni (p. 280)
|
| Geriatric horse (p. 286) | - Strangulating pedunculated lipoma (p. 209) (small intestine or small colon)
- Large colon impaction (p. 217)
|
| Pregnant mare (p. 282) | - Uterine torsion (p. 282)
- Large colon displacement (p. 220)
- Large colon volvulus (p. 220)
- Uterine artery hemorrhage (p. 282)
- Large colon impaction (p. 217)
- Parturition
- Discomfort associated with pregnancy
|
| Postpartum mare (p. 284) | - Large colon volvulus (p. 220)
- Postpartum hemorrhage including uterine artery hemorrhage (p. 284)
- Intestinal ischemia associated with mesenteric rent (p. 284)
- Small colon injury (p. 284)
- Uterine involution
|
| Stallion (p. 285) | - Inguinal hernia (p. 28, 199)
|
| Miniature horse (p. 287) | - Small colon fecalith (p. 287)
- Large colon impaction (p. 217)
- Trichobezoar (p. 287)
|
| Yearling | - Ileocecal intussusception (p. 213)
|
| Weanling (p. 280) | - Ascarid impaction (p. 208, 280)
|
Obtaining the patient’s history
Obtaining a thorough and accurate yet succinct patient history is one of the most important and perhaps one of the more difficult aspects of evaluating the colic patient (Table 1.2). It involves asking a few initial key questions of the owner/caregiver, keeping the owner/caregiver focused on answering the questions thoroughly and concisely during an often stressful situation, and then recognizing areas of the patient’s history that require a more in-depth discussion that may take place following the examination.
Table 1.2 Pertinent questions to be asked of the owner/caregiver for the equine colic patient.
Initial history
- What specific signs is your horse showing?
- What is the duration of time over which your horse has been showing these signs? Have the signs changed over this time?
- What is the reproductive status of the horse?
Appetite, water consumption, defecation, urination
- Has the horse’s appetite and water consumption been within normal limits?
- Has the horse urinated or defecated recently? When was the last time? What was the consistency of feces?
Management
- What is the duration of time the horse has been under the current ownership?
- What is the horse’s current feeding regimen? Dental care?
- What is the horse’s water source?
- Is the horse stalled or on pasture?
- What is the horse’s exercise regimen? What is the intended use of the horse?
- Has there been any change in diet, water source, housing, or exercise regimen?
- Has the horse traveled recently? Where and when?
- What is the horse’s vaccination and deworming history?
Medical history
- Has the horse had signs of colic previously? Previous colic surgery?
- Does the horse have any other medical problems?
- Is the horse currently being treated with any medication? Has any medication been administered for this episode of colic?
- Has the horse had a previous surgical procedure?
- Are the other horses on the farm healthy?
- Does the horse have any stable vices such as crib biting or windsucking?
|
Meticulous medical records need to be maintained with the historical information. Having a standardized history sheet for horses with colic can assist in obtaining a complete history with each case. Further, owners may be able to complete some parts of the history form while the physical examination is being performed (Figure 1.1).
While history taking is traditionally incorporated into the first part of the patient evaluation, it is important to recognize that the entire history does not need to be obtained prior to examining the patient particularly if the patient is showing severe colic signs. However, there are a few very pertinent historical facts that may alter your initial approach to patient care:
- Specific signs being demonstrated by the patient
- Duration of colic signs
- Reproductive status of mares
Initial history
Specific signs
The owner/caregiver should be able to describe specifically the signs being demonstrated by the horse or foal. The term “colic” is often used to describe any equine patient that is “not quite normal“. Recumbency and signs of dull mentation and inappetence are often described as colic. While these signs may be associated with colic, other disease processes should also be considered. Persistent recumbency is more typical of a horse with neurological disease (e.g., equine herpes virus, botulism, or cervical spinal cord injury), severe laminitis, trauma with musculoskeletal injury, debility, or shock from other causes (e.g., blood loss). Dull mentation and inappetence can be associated with any systemic disease process (e.g., colitis, pleuropneumonia, hepatic or renal disease) as well as problems of the head and neck regions.
Signs specific for the horse with colic include pawing at the ground, flank staring, kicking at the abdomen, and rolling. If the horse is not showing any of these signs, the horse is likely to have another problem rather than colic. Colic signs are often described as mild, moderate, or severe:
- Mild colic signs include intermittent flank staring and kicking at the abdomen, inappetence, lying down, and occasional rolling.
- Moderate signs include more persistent rolling but the horse can be distracted and remains standing when walked. The horse may be sweating.
- Severe signs of colic are persistent rolling and thrashing, with difficulty keeping the horse standing when it is walked. The horse is generally covered in sweat and often has multiple abrasions to its head, tuber coxae, and limbs.
Clinical signs shown by the horse should also be interpreted with regard to...