![]()
1
Applied Anatomy of the Ear
The Ear
The ear has three divisions:
1 The outer (external) ear
2 The middle ear
3 The inner ear
External Ear
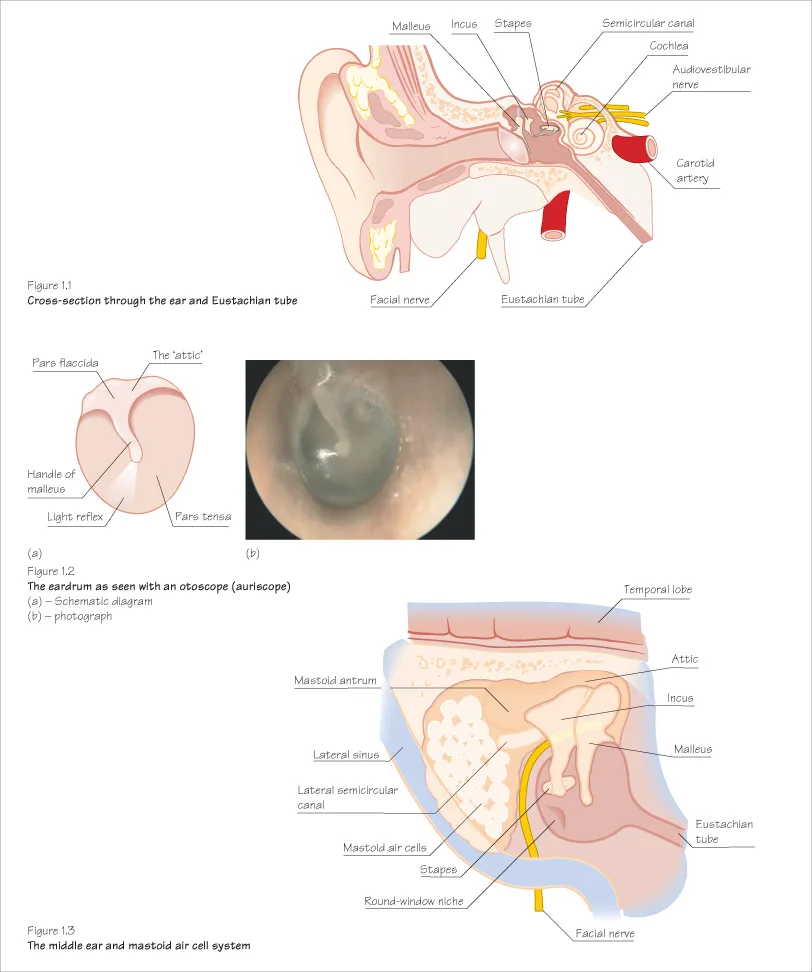
The external ear is made up of (Figure 1.1):
- The pinna
- The external auditory meatus (ear canal)
- Lateral portion of tympanic membrane (ear drum)
The outer (lateral) part of the external ear has a cartilaginous skeleton and the deep (medial) part has a bony skeleton: both are lined by skin. Skin overlying the lateral portion contains hair follicles and sebaceous and wax glands, which are all absent in the medial portion.
The tympanic membrane forms a boundary between the external and middle ears and is divided into the stiffer pars tensa below and the less rigid pars flaccida above (Figure 1.2).
Middle Ear
The middle ear is an air-filled space behind the tympanic membrane that contains the ossicles (bones of hearing): malleus, incus and stapes (Figures 1.1 and 1.3). The ossicles form the ossicular chain, which amplifies and transmits sound vibrations to the inner ear.
The Eustachian tube forms a link between the middle ear and nasopharynx. The facial nerve (cranial nerve VII) also runs through the middle ear. Posteriorly, the mastoid air cell system also opens directly into the middle ear (Figures 1.1 and 1.3).
Inner Ear
The inner ear comprises (Figure 1.1):
- The part of the middle ear behind the pars flaccida is called the ‘attic’.
- The cochlea – this part of the inner ear creates electrical impulses in the cochlear nerve (cranial nerve VIII). These impulses are relayed to the brain to be perceived as sound.
- The vestibule and labyrinth (semicircular canals) – these are involved in balance control.
Anatomical Relations of the Ear
The ear is close to some important structures which can be involved if infection or disease spread:
- Eustachian tube (Figures 1.1 and 1.3) This is a part bony and part cartilaginous tube lined with ciliated epithelium that connects the middle ear space with the nasopharynx. Infection in the nose and pharynx can easily track up this tube to the middle ear, which is really a part of the upper respiratory tract. The Eustachian tube is especially important in children – it is wider, shorter and more upright than in adults. Gently hold your nose, close your mouth and try to exhale – you will feel air entering your middle ear via the Eustachian tube.
- Mastoid air cell system The mastoid process is a bony lump behind the pinna that contains a honeycomb network of epithelium-lined air cells (mastoid air cells). The mastoid air cell system opens directly into the middle ear cleft (Figure 1.3). Infection can track in here to cause ‘mastoiditis’ (see Figure 8.3).
- Middle cranial fossa This contains the temporal lobe of the brain and sits just above the middle ear so meningitis and brain abscess are possible complications of ear infection.
- Venous sinuses These surround the brain and carry blood to the neck veins and are also closely related to the middle ear and mastoid. Infection can propagate and result in potentially fatal cavernous sinus thrombosis.
- Facial nerve The seventh cranial nerve runs through the mastoid and the middle ear. It supplies the muscles of facial expression and is at risk in ear infections and in some types of ear surgery.
TIPS FOR EAR EXAMINATION
- Look at the pinna and the mastoid and check for swellings, scars and colour change.
- Use a good quality otoscope (auriscope) to obtain a view of the eardrum. Use the biggest speculum that will comfortably fit and do not put it in too far.
- You may need to straighten the ear canal by pulling the pinna upwards and backwards to help fit the speculum in.
- Note the condition of the skin of the external ear and try to get a good look at the eardrum in a systematic manner.
- Complete examination includes tuning fork tests, hearing assessment, assessment of facial nerve function and post-nasal space examination to look at the Eustachian tube opening.
Clinical Practice Point
If you cannot obtain a good view of the eardrum using an otoscope, gently manipulate the pinna. Do not put the speculum in too far.
![]()
2
Physiology of Hearing
The ear has two physiological functions: hearing and the maintenance of balance (see Chapter 12).
Physiology of Hearing
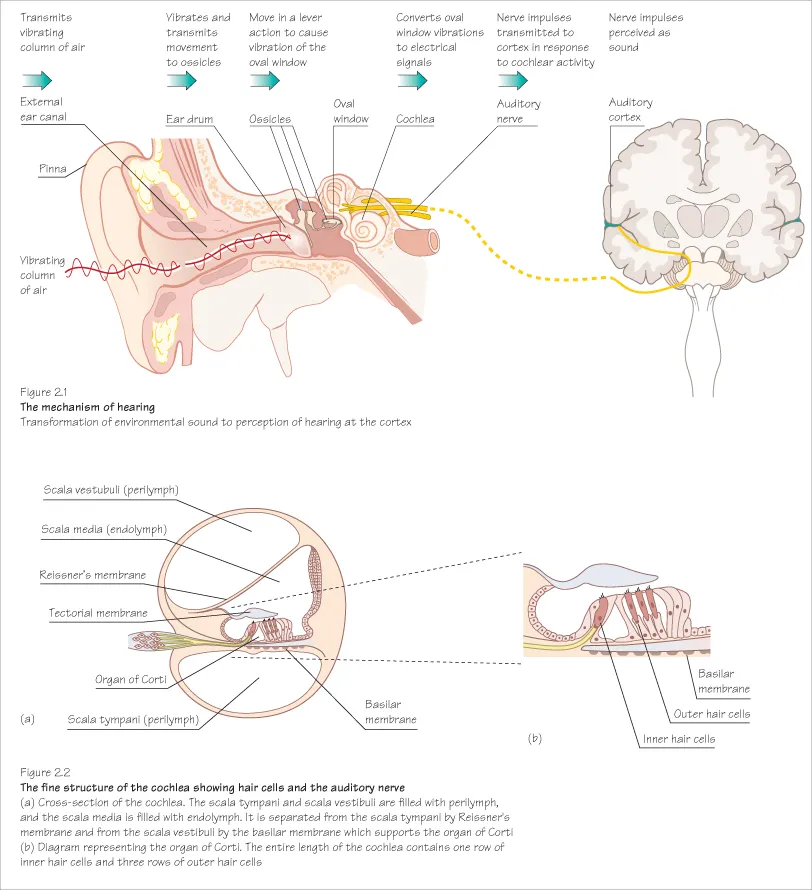
‘Hearing’ is a vital part of our communication; speech, conversation, music, traffic and a host of other sounds are an integral part of our lives. Hearing is a complex physiological process starting with sound energy vibrating a column of air in the external ear and the bones that surround the ear. This in turn causes the eardrum and the attached ossicles to move in a delicate sequence and set up fluid movements in the cochlea or inner ear (Figure 2.1).
Highly specialised cells in the cochlea (hair cells) create electrical impulses that are then transmitted via the auditory nerve to the auditory cortex – the part of the brain concerned with receiving and interpreting sound (Figure 2.2).
This sequence can be interrupted at many levels, causing varying degrees of deafness.
Types of Hearing Loss
Conductive Hearing Loss
Interruption to the hearing mechanism in the external ear or the middle ear prevents ‘conduction’ of sound energy to the cochlea resulting in hearing loss (conductive hearing loss). If the cochlea is working well, vibrations from the environment will still get to the inner ear and the auditory nerve. Some hearing (often quite good hearing) is therefore still possible.
Sensorineural Hearing Loss
If the hearing process is interrupted at the cochlea or in the auditory nerve – for example, if the hair cells are damaged – then the hearing loss is referred to as ‘sensorineural’. It can be complete (i.e. the patient is profoundly deaf), and is much more difficult to treat.
Clinical Practice Point
Always try to distinguish between conductive and sensorineural hearing loss. Tuning fork tests will help but definitive audiometric assessments such as pure tone audiometry are essential (see Chapter 3).
![]()
3
Testing the Hearing
Voice tests and tuning fork tests are easily carried out in a doctor’s office with little or no equipment.
Voice Tests
A good idea of how well a patient hears can be established through simple observation – can he/she hear normal conversational voice or do you have to raise your voice to make yourself clear? If a patient is deaf, you need to know roughly how much and what type (conductive, sensorineural or mixed) of hearing loss he/she has (see Chapter 4). Simple voice/whisper tests can be conducted for a crude assessment of hearing level.
Tuning Fork Tests
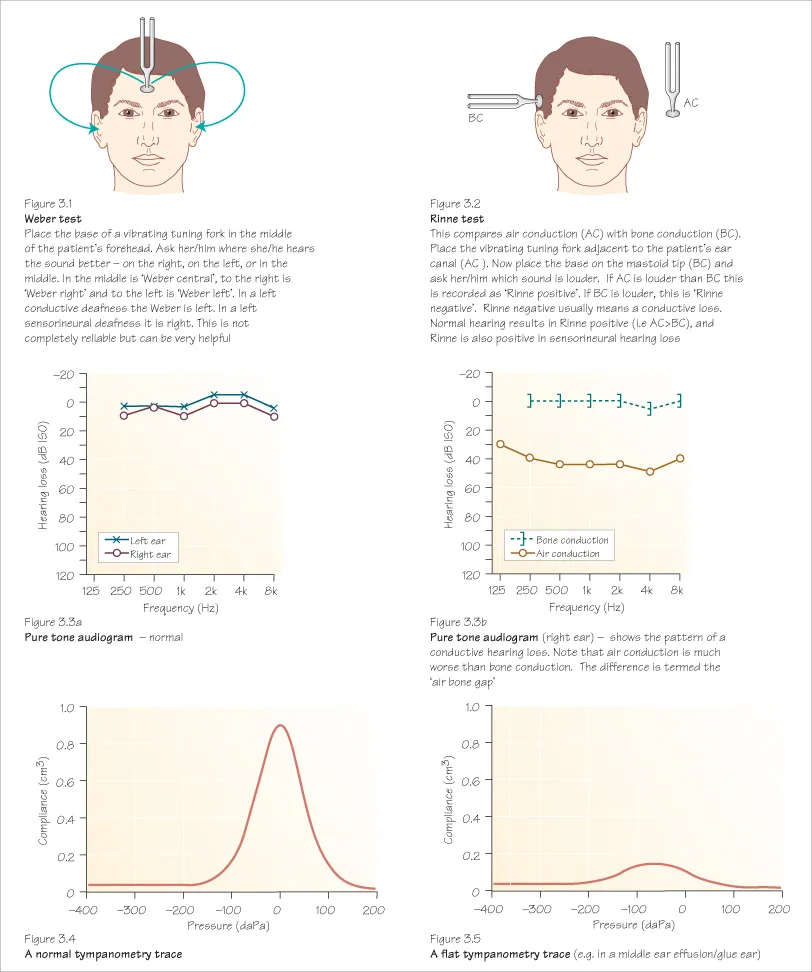
Tuning fork tests can help with lateralising deafness and with deciding which type of hearing loss is present (Figures 3.1 and 3.2).
TIPS FOR TUNING FORK TESTS
- Use a 512-KHz fork with a good heavy base.
- If the hearing is equal in both ears, the Weber test will not lateralise to one side (i.e. the patient will hear the sound in the middle).
- If the Weber is to one side, this can indicate that the other side has little or no hearing, or that there is a conductive deafness on the side the patient identifies as better. Try it yourself – put your finger firmly in the external canal of your own ear and place the tuning fork on your head; you should hear it louder on the side you have blocked as you have given yourself a mild conductive hearing loss.
- The Rinne test is negative if the patient hears the sound better by bone conduction. Usually this means there is a conductive loss on that side.
- Be careful interpreting the Rinne test if the patient has profound hearing loss on one side. A Rinne negative may be because he/she hears sound transmitted across t...