eBook - ePub
Clinical Cases in Orthodontics
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinical Cases in Orthodontics
About this book
Wiley-Blackwell's Clinical Cases series is designed to recognize the centrality of clinical cases to the profession by providing actual cases with an academic backbone. Clinical Cases in Orthodontics applies both theory and practice to real-life orthodontic cases in a clinically relevant format. This unique approach supports the new trend in case-based and problem-based learning, thoroughly covering topics ranging from Class I malocclusions to orthognathic surgery. Highly illustrated in full color, Clinical Cases in Orthodontics' format fosters independent learning and prepares the reader for case-based examinations.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Clinical and Cephalometric Analysis
Introduction
Orthodontics is the area of dentistry concerned with the management of deviations from normal occlusion or malocclusion and involves treatment of children, adolescents and, increasingly, adults. Malocclusion is a variation on normal occlusion and is not a disease entity. Consequently, orthodontic planning and management does not involve binary decisions, but rather evaluation of a range of possibilities to decipher the most appropriate option for each individual.
An ideal static occlusion is characterized by class I molar and incisor relationships, with well-aligned teeth. An acceptable occlusion, however, develops naturally in only 30–40% of the population in Western societies. The occurrence of an acceptable occlusion is multi-factorial, although important factors include the size of the jaws; the relationship of the jaws to each other; the size, number and morphology of the teeth; and the morphology and behaviour of the lips, tongue and peri-oral musculature.
Given that malocclusion does not represent a pathological process but rather a variation from an accepted norm, there is little agreement, even among orthodontists, as to when orthodontic treatment becomes necessary (Richmond et al., 1984). As a consequence, a variety of orthodontic indices have been developed to ration treatment where care is provided as part of a public health service, such as in the UK and Scandinavia (Brook and Shaw, 1989), based primarily on aesthetic and dental health impairment.
The demand for orthodontic treatment has increased universally, particularly over the past two decades. A desire to enhance dental appearance is the underlying motivation for most patients who seek orthodontic treatment (Shaw et al., 1991). Furthermore, the lay public has developed an increasing awareness of the importance of the dentition to overall attractiveness. Carefully planned and well-executed orthodontics can also enhance facial appearance, which in turn has been linked to improved social skills, greater desirability, higher intellectual ability and enhanced occupational prospects (Shaw et al., 1979).
Deviation from occlusal norms may leave children susceptible to harassment, teasing and bullying, with obvious psychosocial implications (Shaw et al., 1980; Seehra et al., 2011). Consequently, orthodontic treatment may have significant psychosocial benefits (Shaw et al., 1980; O’Brien et al., 2003) and can often lead to improved oral health-related quality of life. Similarly, combined orthodontic–surgical treatment has been linked to notable enhancement of both self-esteem and quality of life (Arndt et al., 1986).
The undoubted benefits of orthondontics are, however, reliant on careful diagnosis, planning and management. Clinical assessment and radiographic analysis are central to the formulation of appropriate treatment decisions leading to the best aesthetic and functional outcome from treatment.
As in any other area of medicine or dentistry, to reach a diagnosis in orthodontics requires a thorough history, examination and special tests. A comprehensive history should be undertaken to clarify the motivation for treatment, the dental and orthodontic history, and any relevant medical history that might impact on the provision of orthodontic treatment (Patel et al., 2009).
Dental History
A history of dental attendance is relevant in relation to caries experience and the presence of restorations. Caries experience is the best predictor of future caries. Poor oral hygiene predisposes to two risks of treatment: gingivitis and demineralization. Premature loss of primary teeth due to caries may also have consequence for the developing dentition. In particular, early loss of primary teeth may hasten or retard eruption of permanent teeth and lead to space loss, which can result in centre line discrepancies or potential tooth impaction.
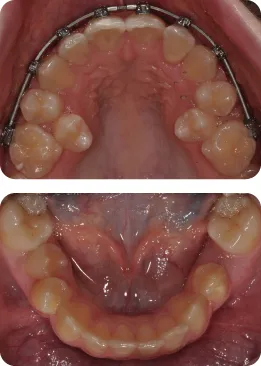
What Has Led to Crowding of the Second Premolars in Figure 1.1?
Early loss of the second primary molars has allowed the first permanent molars to drift forward in the dental arch. The second premolars are most vulnerable to space loss in this region.
Figure 1.1
Restorations
Heavily-restored teeth may pose problems in relation to bonding, necessitating alteration of the bonding protocol, with sandblasting of amalgam and precious metal restorations proven to enhance bond strength (Zachrisson et al., 1995; Büyükyilmaz et al., 1995). There is conflicting evidence in relation to the susceptibility of root canal-treated teeth to root resorption during treatment. Nevertheless, the health of root-treated teeth should be monitored throughout treatment.
Trauma
A history of trauma to the dentition should be investigated. Previously traumatized teeth risk loss of vitality irrespective of orthodontic treatment. This potential eventuality should be discussed at the outset as part of the informed consent process. In addition, traumatized teeth may also be at risk of undergoing more apical root resorption during treatment. The nature and timing of the traumatic injury has a bearing on further treatment (Kindelan et al., 2008) (Table 1.1).
Table 1.1 Timing of further treatment for traumatic injury
| Type of injury | Recommended observation period before orthodontic treatment |
| Fracture without pulpal involvement | 3 months |
| Subluxation | 3 months |
| Extrusive luxation | 3 months |
| Minor lateral luxation | 3 months |
| Moderate/severe lateral luxation | 1 year |
| Intrusion | 1 year |
| Avulsion | 1 year |
Previous Orthodontics
Increasingly, potential orthodontic patients, particularly adults, may have undergone previous treatment. Details of the original malocclusion may help to decipher the aetiology of both the presenting and residual malocclusion. Potential consequences of incomplete treatment include residual malalignment and spacing, traumatic overbite, residual overjet, crossbite and relapse. Previous failure to complete a course of orthodontic treatment may raise questions with respect to compliance (Murray, 1989). Where compliance is questionable, it may be inadvisable to embark on an ambitious course of orthodontic treatment.
Furthermore, contemporaneous records are important to reveal deleterious effects of the primary phase. Rarely, significant root resorption may limit the feasibility for retreatment.
CASE 1.1
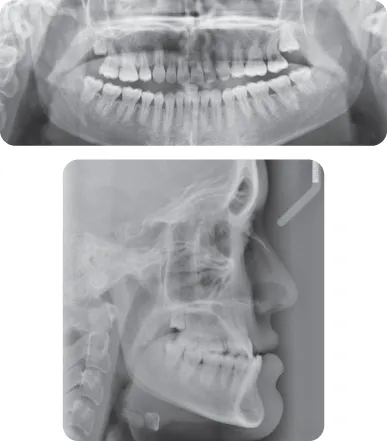
This 17-year-old female presented with a class III malocclusion on a moderate skeletal class III pattern with an average lower facial height. She has had previous orthodontic treatment to align her maxillary teeth, involving extraction of maxillary first premolars. She remains concerned in relation to her facial appearance and occlusion.
What Do You Notice with Respect to the Radiographic Appearance of the Maxillary Incisors (Figure 1.2)?
The maxillary incisors, particularly the UR1, UL1 and UR2, have experienced extensive root resorption during the first phase of treatment.
Figure 1.2
How Will This Finding Influence Further Management?
The patient is keen to undergo combined orthodontic–surgical treatment to address her malocclusion comprehensively. Prior to instituting such treatment, the patient will be counselled in relation to the likelihood of further resorption. If the patient opts to undergo combined treatment, attempts will be made to avoid an upper fixed appliance. If an appliance is to be placed, light forces will be applied, there will be a premium on excellent oral hygiene and the duration of treatment will be necessarily short with realistic objectives.
Family History
The contribution of genetic factors to malocclusion has been established in family and twin studies. Concordance of occlusal patterns in monozygotic twins pr...
Table of contents
- Cover
- Title page
- Copyright page
- Acknowledgements
- Preface
- 1 Clinical and Cephalometric Analysis
- 2 The Developing Dentition
- 3 Class I Malocclusion
- 4 Class II Division 1 Malocclusion
- 5 Class II Division 2 Malocclusion
- 6 Class III Malocclusion
- 7 Tooth Impaction
- 8 Fixed Appliances
- 9 Stability and Retention
- 10 Orthognathic Surgery
- 11 Development of the Craniofacial Region
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Cases in Orthodontics by Martyn T. Cobourne,Padhraig S. Fleming,Andrew T. DiBiase,Sofia Ahmad in PDF and/or ePUB format, as well as other popular books in Medicine & Orthodontics. We have over 1.5 million books available in our catalogue for you to explore.