![]()
Section II
Common Child and Adolescent Psychiatric Disorders
![]()
10
Attention-Deficit Hyperactivity Disorder
David M. Rube, Tejal Kaur
Introduction
Attention-deficit hyperactivity disorder (ADHD) is one of the most common neuropsychiatric conditions of childhood and adolescence, and is also one of the best researched neurobiological conditions in medicine, with over 200 placebo-controlled medication trials displaying acute response [1]. The core symptoms of ADHD are manifest throughout the life cycle, from preschool through adult life; they interfere with a child's family and peer interactions, academic attainment, emotional development, self-esteem, and overall quality of life. Given the high prevalence, impairment, and societal cost of ADHD, treatment is not only essential, but also practical and efficacious.
History
In North America, children who survived the great encephalitis epidemics of 1917 and 1918 were noted to have many behavioral problems similar to those constituting what we call ADHD [2, 3]. The cases that were reported and others that have arisen due to birth trauma, head injury, exposure, or infections gave rise to the idea of a “brain-injured child syndrome.” This concept evolved into that of minimal brain damage and eventually minimal brain dysfunction. Many challenges were raised to this label, however, because of the lack of evidence of brain injury in many of the children who exhibited the symptoms.
In the late 1950s and early 1960s, the “hyperactive child syndrome” was described by Burks and Chess [4, 5]. That syndrome was typified by daily movement that was greater than that of normal children of the same age. In the late 1960s, under the influence of the psychoanalytic movement, the second edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-II) [6] described all childhood disorders as “reactions,” and the hyperactive child syndrome became the “hyperkinetic reaction of childhood.” It was defined as a disorder of overactivity, restlessness, distractibility, and short attention span. It was asserted that the behavior usually diminishes in adolescence, leading to the ongoing myth that ADHD “disappears in adolescence.”
In the revised edition of DSM-III (DSM-III-R) [7], the disorder was renamed ADHD (attention deficit hyperactivity disorder), with a single list of items incorporating all three symptoms and a single threshold for diagnosis. Since the publication of the DSM-III-R, researchers have found that the problems with hyperactivity and impulsivity were not separate but formed a single dimension of behavior. These conclusions led to the creation of two separate symptom lists when DSM-IV was published in 1994 [8]. The establishment of the inattention list once again permitted the diagnosis of a subtype of ADHD. The DSM-IV currently permits diagnosis of subtypes of attention-deficit hyperactivity disorder: inattentive type, hyperactive impulsive type, and, for children with problems from both lists, ADHD combined type.
Core Clinical Criteria
For a diagnosis of ADHD, DSM-IV requires an early age of onset (prior to age 7 years), the presence of impairment for 6 months or longer, and the presence of impairment in two or more settings (see Table 10.1). Inattention includes failing to give close attention to details, difficulty sustaining attention, not listening, not following through, difficulty organizing, losing things, becoming easily distracted, and forgetfulness. Hyperactivity includes fidgeting, being out of seat, running or climbing excessively, having difficulty playing quietly, being “on the go” or as if “driven by a motor,” and talking excessively. The impulsivity symptom criteria include blurting out answers, having difficulty awaiting a turn, and often interrupting or intruding on others [8]. Core deficits include impairment in rule-governed behavior across a variety of settings and relative difficulty for age in inhibiting an impulsive response to internal wishes, needs, or external stimuli.
Table 10.1 Criteria for the diagnosis of attention-deficit hyperactivity disorder (ADHD).
|
| The diagnosis requires evidence of inattention or hyperactivity and impulsivity or both |
| Inattention |
| Six or more of the following symptoms of inattention have persisted for at least six months to a degree that is maladaptive and inconsistent with developmental level: |
| Often fails to give close attention to details and makes careless mistakes |
| Often has difficulty sustaining attention |
| Often does not seem to listen |
| Often does not seem to follow through |
| Often has difficulty organizing tasks |
| Often avoids tasks that require sustained attention |
| Often loses things necessary for activities |
| Often is easily distracted |
| Often is forgetful |
| Hyperactivity and impulsivity |
| Six or more of the following symptoms of hyperactivity and impulsivity have persisted for at least six months to a degree that is maladaptive and inconsistent with developmental level: |
| Often fidgets |
| Often leaves seat |
| Often runs about or climbs excessively |
| Often has difficulty with quiet leisure activities |
| Often is ‘on the go’ or ‘driven by a motor’ |
| Often talks excessively |
| Often blurts out answers |
| Often has difficulty awaiting turn |
| Often interrupts or intrudes |
| Symptoms that cause impairment: |
| Are present before seven years of age |
| Are present in two or more settings (e.g., home, school, or work) |
| Do not occur exclusively during the course of a pervasive developmental disorder, schizophrenia, or another psychotic disorder |
| Are not better accounted for by another mental disorder (e.g., a mood disorder or an anxiety disorder) |
While the syndrome may manifest itself differently throughout the life cycle, school-age children are the most common presenting population to pediatricians, child psychiatrists, and psychologists. Weiss [9, 10] points out that these children typically present with:
- inappropriate or excessive activity, unrelated to the task at hand, which generally has an intrusive or annoying quality;
- poor sustained attention;
- difficulties in inhibiting impulses in social behavior and cognitive tasks;
- difficulties getting along with others;
- school underachievement;
- poor self-esteem secondary to difficulties getting along with others and school underachievement;
- other behavior disorders, learning disabilities, anxiety disorders, and depression.
Restlessness is measured by well-standardized rating scales and direct and indirect observation [11, 12]. Teachers and parents may not agree with one another, owing to the likelihood that children may act differently in different situations, particularly as the full range of ADHD symptoms are less likely to emerge in settings where a child likes a teacher or tries harder at home to please his or her parents. Consequently, a child being evaluated in a physician's office could sit perfectly still during the examination, and the clinician may use rating scales in settings where the child spends the majority of his time. Whalen and Henker [13] suggest that “each measure reflects a unique child × perceiver × setting example.”
Bewildered parents will report their child's difficulties with attention. A common complaint is “he can play video games for hours but to do 20 minutes worth of homework requires 1 to 2 hours worth of screaming and temper tantrums.” It seems that when a particular activity interests a child, he or she can pay attention for hours. However, these same children can have a poor attention span when attending to tasks they find boring, repetitive, or difficult and that give them no satisfaction.
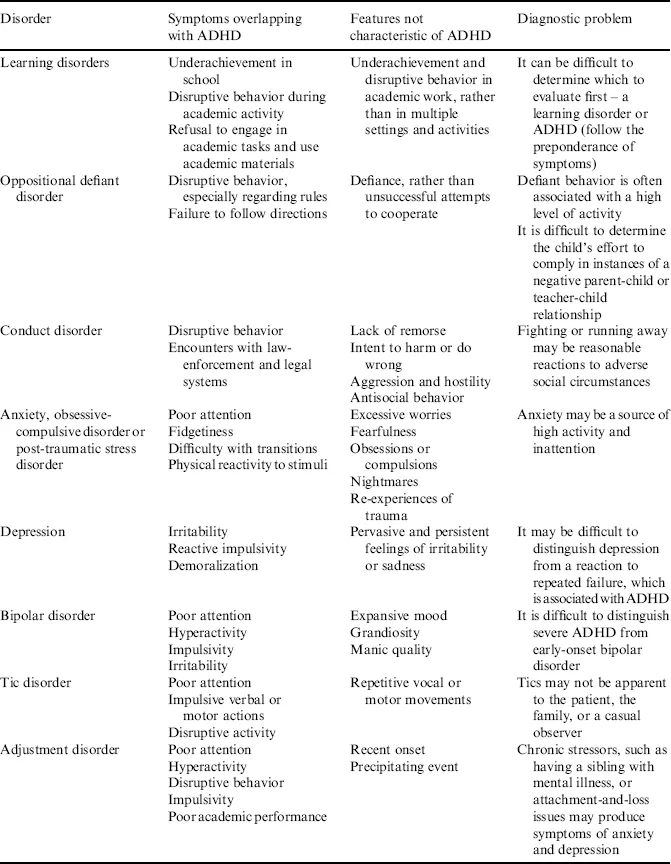
Poor attention span should be carefully assessed, as it can also be very similar to the poor concentration seen in anxiety and mood disorders. Moreover, as many of the core symptoms of ADHD can appear cross-sectionally to mimic other Axis I psychiatric diagnoses, and vice versa, a thorough assessment should begin with a broad-based differential (see “Differential Diagnoses” and Table 10.2).
Table 10.2 Mental health conditions that mimic or coexist with attention-deficit hyperactivity disorder (ADHD).
Difficulty Getting Along with Others
Peers often quickly reject children with ADHD because of their aggression, impulsivity, and noncompliance with rules [14]. Children with ADHD may be unpopular with their peers and may have difficulties with parents, siblings, and teachers [15]. These children may have few “best friends” and few enduring friendships, and this unpopularity and inability to establish and maintain friendships may be replaced in life by social isolation. In childhood, sometimes the only person willing to play with a hyperactive child is a younger child or a child with some other similar difficulty.
The negative effect of hyperactive children on others has been observed with respect to their teachers and ability to participate in both dyads and groups of children. Parents may also interact with a hyperactive child in a more negative and intrusive way. Furthermore, as ADHD often runs in families, one often discovers the likelihood that the parent may also have significant ADHD symptoms, which contribute to general disorganization in the household, which in turn often exacerbates ADHD and concomitant behavioral symptoms. Although working with parents to increase structure and behavioral modification strategies at home can prove beneficial, simultaneous addition of medication can lead to improved relationships with peers, teachers, and parents.
School Underachievement
Cantwell and Baker [16] showed that even when intelligence was controlled for, hyperactive children were behind normal children in their grade level in reading, spelling, and arithmetic. Even in the absence of comorbid learning disorder, t...