![]()
1
Trigeminal Neuralgia
Maarten van Kleef, Wilco E. van Genderen, Samer Narouze, Turo J. Nurmikko, Jan Van Zundert, José W. Geurts and Nagy Mekhail
Introduction
“Trigeminal Neuralgia is the worst pain in the world,” declared Peter J. Jannetta, MD in “Striking Back!”, a layman’s guide for facial pain patients.1 Trigeminal neuralgia, or “Tic Doloureux”, is a painful condition of the face. This pain has been known since ancient times; there are descriptions of facial pain by Ibn Sina (980–1073) in an Arabic text. An example of early interventional treatment is that by Locke in 1677, who applied sulphuric acid to the face of the Duchess of Northumberland in an attempt to treat her trigeminal neuralgia.
A survey conducted in 6 European countries indicated that trigeminal neuralgia significantly impacted the quality of life and the socioeconomic functioning of affected patients.2 Trigeminal neuralgia is the most common form of facial pain in people older than 50 years of age. Various epidemiological studies have shown the annual incidence to be about 4–5 new patients per 100,000. The highest incidence occurs in the ages between 50 and 70 years; in 90% of the cases the symptoms begin after the age of 40 years. Trigeminal neuralgia is more prevalent in women than men with a ratio of 1.5:1.3
The pathophysiology is unclear. Based on clinical observations, compression of the nervus trigeminus near the origin of the brain stem, the so-called root entry zone, by blood vessels or tumor, may cause trigeminal neuralgia. Local pressure causes demyelination that leads to abnormal depolarization resulting in ectopic impulses.
Symptoms
Trigeminal neuralgia is recognized by unilateral short-lived, strong, sharp, shooting pains in 1 or more branches of the fifth cranial nerve. The description of the pain is very important; it must be sharp, shooting, lancinating, and “electric shock”. The pain can be brought on by ordinary stimuli, such as eating, washing, shaving, cold, warmth, and draught. The distribution of the pain in the various branches of the nervus trigeminus is given in Table 1.1.
Table 1.1. Pain distribution in the various nerve branches in trigeminal neuralgia.
See Rozen.3
| V1 only | 4% |
| V2 only | 17% |
| V3 only | 15% |
| V2 + V3 | 32% |
| V1 + V2 | 14% |
| V1 + V2 + V3 | 17% |
In the case history, 6 questions should be asked:
1 Does the pain occur in attacks?
2 Are most of the attacks of short duration (seconds to minutes)?
3 Do you sometimes have extremely short attacks?
4 Are the attacks unilateral?
5 Do the attacks occur in the region of the nervus trigeminus?
6 Are there unilateral autonomic symptoms?
In this way, a differential diagnosis can be made relatively quickly and an impression can be formed of whether it is essential trigeminal neuralgia.
Physical Examination
Neurological examination seldom reveals any abnormalities in patients with idiopathic trigeminal neuralgia, but all cranial nerves do need to be tested. Patients who have neurological disorders often have a so-called secondary trigeminal neuralgia whereby the trigeminal neuralgia is a symptom of another disease, e.g., tumor of the angulus pontocerebellaris or multiple sclerosis.
Additional Test
When the diagnosis of trigeminal neuralgia is made, the patient needs to undergo an magnetic resonance imaging (MRI) scan to exclude specific pathologies such as a tumor or multiple sclerosis, which could cause a secondary trigeminal neuralgia. The MRI scan can also be used if there is a suspected compression of the nervus trigeminus in the fossa cranialis posterior. Sometimes the MRI scan is sensitive enough to detect blood vessels that have come in contact with the nervus trigeminus. The role of venous compression in the pathogenesis of trigeminal neuralgia is controversial.4,5 Notably, on MRI scanning, compressing blood vessels are seen in one-third of asymptomatic patients. A recent evidence-based review concluded that there is insufficient evidence to support or deny the usefulness of MRI to identify neurovascular compression.6
Differential Diagnosis
Less frequently trigeminal neuralgia is seen in younger patients. It is important that multiple sclerosis always be considered in the differential diagnosis, especially in bilateral cases. The International Headache Society described the following criteria for essential trigeminal neuralgia.7
A Paroxysmal pain that lasts from a fraction of a second to 2 minutes, occurring in 1 or more branches of the nervus trigeminus, and fulfilling criteria B and C.
B The pain has at least one of the following characteristics:
1 intense, sharp, superficial or stabbing.
2 precipitated from trigger areas or by trigger factors.
C The attacks are stereotypically described by the patient.
D There are no signs of neurological disorders.
E The attacks are not caused by other disorders.
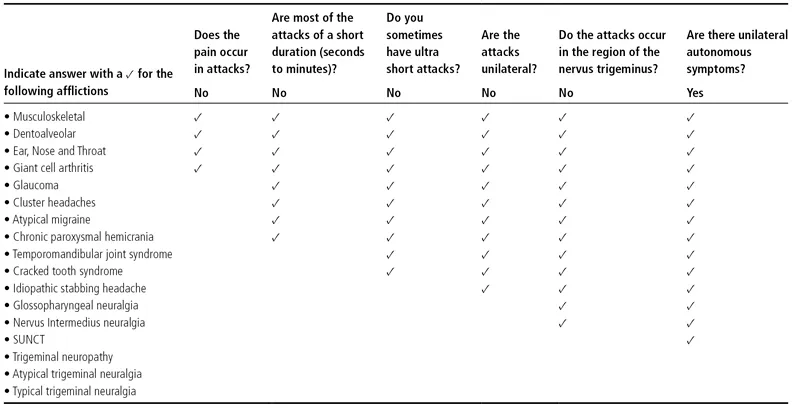
The International Headache Society have suggested their own diagnostic criteria for trigeminal neuralgia (Table 1.2).8 The differential diagnosis of essential trigeminal neuralgia is extensive and involves all unilateral pain in the pathway of the nervus trigeminus. The most important differential diagnostic considerations are specific facial pain, nonspecific facial pain, temporomandibular arthrosis, dental disorders, and vascular migraine. A detailed overview of the differential diagnosis of facial pain can be found in Table 1.3.9
Table 1.2. Trigeminal neuralgia: clinical diagnostic criteria.
|
| Character | Shooting, like an electric shock, stabbing, superficial |
| Seriousness | Moderate to very intense |
| Duration | Each pain attack lasts seconds but a number of different attacks can occur simultaneously after which there is a pain free interval |
| Periodicity | Periods of weeks to months without pain |
| Location | Distribution of T. neuralgia, mainly unilateral |
| Emanation | Within the area of the trigeminal nerve |
| Trigger factors | Light touching, such as when eating, talking or washing |
| Alleviating factors | Frequent sleep, anti-epileptics |
| Accompanying characteristics | Trigger zones, weight loss, poor quality of life, depression |
Table 1.3. Differential diagnosis of trigeminal neuralgia.
See Nurmikko.32
Treatment Options
Conservative Treatments
The selection of the pharmacological treatment is based on a systematic review of data of relatively older studies10 or on a more up-to-date Cochrane database.11 The medication of choice is carbamazepine. From an observational study, it appears that carbamazepine can reduce the pain symptoms in about 70% of the cases. Oxcarbazepine has shown similar efficacy.6 Other medications that can be tried, although there is no clinical evidence for their efficacy, are gabapentin, pregabalin, and baclofen. Rozen summarized the recommendations for the medical treatment of trigeminal neuralgia in Table 1.4.3
Table 1.4. Medical treatments for trigeminal neuralgia.
See Rozen.3...