![]()
1
Sinus Rhythm
The sinus node lies at the junction of the superior vena cava and right atrium. Atrial activation travels inferiorly from the sinus node to the atrioventricular (AV) node, resulting in a positive P wave in the inferior ECG leads, II, III and aVF. If the QRS complex is preceded by a P wave that is not positive in the inferior leads then the rhythm is other than sinus rhythm. The sinus node impulse is conducted relatively slowly via the AV node to reach the His–Purkinje system, which then conducts very rapidly to activate the ventricular myocardium.
Normal sinus rhythm is characterised by a rate of 60–100 beats/min; PR interval 0.12–0.21 s; QRS duration ≤ 0.10 s; QTc ≤ 0.44 s.
ECG characteristics
The sinus node initiates the electrical impulse that activates atrial and then ventricular myocardium during each normal heartbeat. Sinus node activity itself does not register on the electrocardiogram (ECG).
P wave
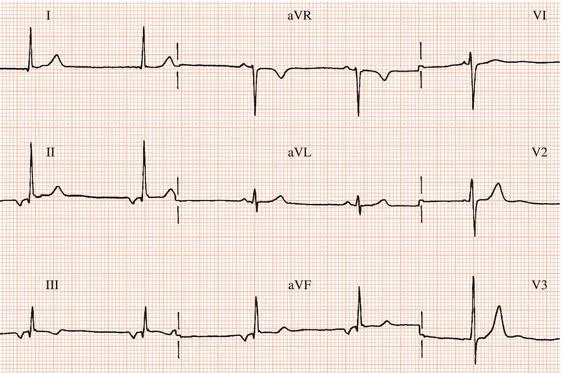
Atrial activity, the P wave, is usually apparent in most ECG leads (Figure 1.1). However, occasionally the P wave in some leads is not visible or is of low amplitude, and it may be necessary to inspect all leads of the ECG to establish that there is sinus rhythm (Figure 1.2).
The sinus node lies at the junction of the superior vena cava and right atrium. Atrial activation therefore spreads from the sinus node in an inferior direction (i.e. towards the feet) to the atrioventricular (AV) junction. The P wave, therefore, is upright in those leads that are directed to the inferior surface of the heart (i.e. II, III and aVF), and is inverted in aVR, which faces the superior heart surface (Figure 1.1). If a P wave does not have these characteristics then, even though a P wave precedes each ventricular complex, the sinus node has not activated the atria and the rhythm is abnormal (Figure 1.3).
PR interval
The AV node is the only electrical connection between atria and ventricles: the mitral-tricuspid valve ring that separates the atria from the ventricles is fibrous and cannot conduct electrical impulses. The AV node conducts relatively slowly, thereby delaying conduction of the atrial impulse to the ventricles. Conduction through the AV node does not register on the ECG. The PR interval, which is measured from the onset of the P wave to the onset of the ventricular complex, indicates the time taken for an atrial impulse to reach the ventricles. The normal PR interval ranges from 0.12 to 0.21 s. It should shorten during sinus tachycardia.
QRS complex
After traversing the AV node, the activating impulse reaches the bundle of His, which divides into the right and left bundle branches. The bundle of His, the bundle branches and their ramifications, the Purkinje fibres, constitute the ‘specialised intraventricular conducting system’ which facilitates very rapid conduction of the impulse through the ventricular myocardium. Ventricular activation (i.e. depolarisation) is represented by the QRS complex, which is normally no greater than 0.10 s in duration. The amplitude of the QRS complex is larger than that of the P wave because the mass of the ventricles is much greater than that of the atria.
T wave
The T wave is the result of the electrical recovery of ventricular myocardium prior to the next heartbeat, i.e. repolarisation. Sometimes, a low-amplitude wave can be seen following the T wave, termed a U wave. It is thought to result from repolarisation of the Purkinje fibres and is usually seen in leads V2–4.
The QT interval, which is measured from the onset of the QRS complex to the end of the T wave, represents the duration of ventricular activation plus recovery. The QT interval normally shortens with increasing heart rate, partly due to the increase in rate itself and partly due to the increase in sympathetic nervous system activity related to sinus tachycardia. When measuring the QT interval it is necessary to correct the measured interval for heart rate. The corrected QT interval (QTc) is calculated by selecting the ECG lead showing the longest QT interval, and then dividing the square root of the cycle length into the measured QT interval. For example, a patient with a measured QT interval of 0.40 s at a heart rate of 60 beats/min has a cycle length of 1.0 s and therefore also has a QTc of 0.40 s. QT prolongation and a prominent U wave are seen in certain hereditary and acquired conditions.
ECG characteristics of normal sinus rhythm
P wave
Precedes each QRS complex
Upright in leads III, aVF
Inverted in lead aVR
PR interval
Duration 0.12–0.21 s
QRS complex
Duration ≤ 0.10 s
QTc interval
Duration ≤ 0.42 s (men), ≤ 0.44 s (women)
Relative speeds of impulse conduction
Appreciation of the relative speeds of impulse conduction through the heart – slowest through the AV node, fastest through the specialised intraventricular conducting system and at an intermediate rate through ordinary working myocardium – is important in understanding the mechanisms of a number of arrhythmias as well as generation of the normal P-QRS complex.
Speed of impulse conduction
His–Purkinje system > myocardium > AV node
Sinus bradycardia
Sinus bradycardia is sinus rhythm at a rate less then 60 beats/min (Figure 1.4). It may be physiological, as in athletes or during sleep, or it may result from acute myocardial infarction, sick sinus syndrome or from drugs such as beta-adrenoceptor blocking drugs (beta-blockers). Non-cardiac disorders such as hypothyroidism, jaundice and raised intracranial pressure can also cause sinus bradycardia.
Atropine, isoprenaline or pacing can be used to increase the rate but are only necessary when sinus bradycardia causes symptoms or marked hypotension, or leads to tachyarrhythmia.
Sinus tachycardia
Sinus tachycardia is defined as sinus rhythm at a rate greater than 100 beats/min (Figure 1.5). Exercise, anxiety or any disorder that increases sympathetic nervous system activity may cause sinus tachycardia.
Occasionally, sinus tachycardia can be inappropriate. Hyperthyroidism is a possible cause. However, often no cause is found. Young females are most commonly affected. Fast rates are usually persistent and there is an exaggerated response to exercise with rates increasing rapidly almost immediately exertion begins. Rarely, inappropriate sinus tachycardia is due to a primary disorder of the sinus node (sinus node re-entry).
Since sinus tachycardia is usually a physiological response, there is rarely a need for specific treatment. However,...