![]()
Chapter 1
Prehospital Emergency Medicine
Matthew Boylan1 and Tim Nutbeam2
1Royal Centre for Defence Medicine, University Hospitals Birmingham, Birmingham, UK
2Derriford Hospital, Plymouth Hospitals NHS Trust, Plymouth, UK
Introduction
‘Prehospital care’ is the term given to the provision of medical care outside of the hospital or alternative fixed healthcare setting. In the developed world, the provision of prehospital care is usually the responsibility of a regional ambulance or emergency medical service (EMS). A number of agencies may operate in support of the ambulance service including private ambulance companies, rescue organizations (e.g. mountain rescue, air ambulance services), the voluntary aid societies (e.g. Red Cross) and immediate care practitioners (e.g. British Association of Immediate Medical Care, BASICS).
Prehospital emergency medicine
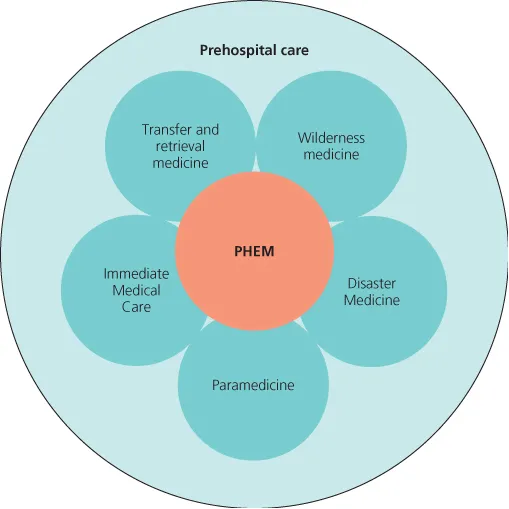
Prehospital emergency medicine (PHEM) is a field within prehospital Care (Figure 1.1). PHEM's evolution has been triggered by the demand to meet new challenges imposed by the regionalization of specialist medical and trauma services. Many of the critically injured or unwell patients that prove to benefit most from these new systems of care are paradoxically those less likely to tolerate extended transfer without advanced critical care support. As a result, there is a need to provide a body of prehospital practitioners capable of providing advanced clinical assessment and critical care intervention at the scene of an incident, together with safe critical care retrieval to an appropriate centre of care. In most continents the enhanced skill set required to provide this level of care falls outside that deliverable by the ambulance service or its supporting bodies, and therefore requires the deployment of specially trained physician-led teams.
The role of the PHEM practitioner or team is to augment the existing prehospital response, not replace it. Their function is to provide an additional level of support for those patients with higher acuity illness and injury, both on scene and during transfer. In doing so they are also well placed to educate and enhance the skills of the prehospital providers they work alongside.
Training in PHEM
An important move forward in the evolution of the field of PHEM in the UK has been its recognition as a new medical subspecialty led by the Intercollegiate Board for Training in prehospital Emergency Medicine (IBTPHEM). IBTPHEM has produced a curriculum that outlines the knowledge, technical skills and non-technical (behavioural) skills required to provide safe prehospital critical care and safe transfer. Links to the IBTPHEM and their curriculum can be found in the further reading section. The key themes of the curriculum are shown in Figure 1.2.
Similar prehospital training programmes exist across Europe (e.g. Germany) where they are firmly integrated into medical training and the emergency medical services (EMS). In Australasia, geography has been the driving force behind the development of retrieval medicine as a specialization. A number of retrieval services (e.g. Greater Sydney Area HEMS) have recognized the commonality between PHEM and retrieval medicine and have moved towards delivering a combined model that provides both interfacility secondary transfer and primary prehospital retrieval. The experiences of many of these systems has helped mould the new PHEM subspecialty within the UK.
Summary
PHEM is a challenging and exciting development within the area of prehospital care. This book aims to provide some of the underpinning knowledge required for effective PHEM practice.
Further reading
IBTPHEM website: www.ibtphem.org.uk.
![]()
Chapter 2
Activation and Deployment
Andrew Thurgood1 and Matthew Boylan2
1Mercia Accident Rescue Service (MARS), UK
2Royal Centre for Defence Medicine, University Hospitals Birmingham, Birmingham, UK
OVERVIEW
By the end of this chapter you should:
- Understand how emergency calls are handled and prioritized
- Understand the different types of dispatch
- Understand the risks and benefits of deployment by road
- Understand the risks and benefits of deployment by air.
Introduction
The first step in delivering high-quality prehospital care is the timely activation and deployment of prehospital resources. The initial aim is to get the right resource to the right patient in the right time frame. This process requires efficient call handling, robust call prioritization and intelligent tasking of resources. Prehospital practitioners may deploy to scene using a variety of different transport modalities. The choice of modality will be determined by the system in which they work and by the nature and location of the incident.
Activation of prehospital services
It is important for the prehospital practitioner to have an understanding of how emergency calls are processed and resources dispatched.
Call handling
In most developed countries there is a single emergency telephone number that members of the public may dial to contact the emergency services. The emergency number differs from country to country but is typically a three-digit number that can be easily remembered and dialled quickly, e.g. 911 in the USA, 999 in the UK and 000 in Australia. In the 1990s the European Union added 112 as the Global System for Mobile Communications (GSM)-approved common emergency telephone number.
Emergency calls from telephone and mobile phones pass to operators within designated Operator Assistance Centres (OACs) run by phone providers. Their function is to determine which emergency service is required and forward the caller details to the appropriate Police, Fire or Ambulance Emergency Control Centre (ECC). In the UK this information is passed electronically in the form of Caller Line Identification (CLI) via a system called Enhanced Information Service for Emergency Calls (EISEC). The data then appears automatically as an incident on the dispatchers computer-aided dispatch (CAD) screen in the ECC (Figure 2.1). While this automatic data transfer occurs, the caller is connected to a call taker at the ECC who will begin the process of call prioritization.
Call prioritization
There are a number of systems by which calls can be prioritized. The most common system used within the UK ambulance service is the Advanced Medical Priority Despatch System (AMPDS). Similar systems of Medical Priority Dispatch are in use within the USA and Australia. AMPDS uses a structured question–answer logic tree to allocate a dispatch priority: Red—Category A (immediately life threatening), Amber - Category B (urgent call), or Green—Category C (routine call). This mode of caller interrogation is known as systematized caller interrogation. AMPDS incorporates protocolized pre-arrival first aid instructions that are relayed by the call taker to the caller while they await the emergency response. In addition, each injury and injury mechanism is allocated a unique AMPDS code for audit purposes.
Although effective in prioritizing an ambulance service response, AMPDS has been shown to lack the sensitivity and specificity required to select calls that would benefit from enhanced prehospital emergency medicine (PHEM) intervention. In order to identify these cases, an additional tier of enhanced caller interrogation and dispatch criterion is required. For maximum efficiency this tier should be delivered by active PHEM practitioners (e.g. critical care paramedics or doctors) as they are in the best position to make accurate judgements about the likely need for advanced interventions. The use of non-clinical dispatchers in this role is associated with high rates of over-triage.
The model operated by London Helicopter Emergency Medical Service (HEMS) in ...