Skin disease can be more than skin deep
Our skin is one of the first things people notice about us. Blemishes, rashes, dry, flaky skin – all these can breed insecurity, even suicidality, even though the basic skin condition is relatively benign. Skin disease can lead to psychiatric disturbance.
But symptoms of skin disease can also indicate psychological disturbance. Scratching, scarring, bleeding, rashes. These skin disturbances can be the result of psychiatric disease.
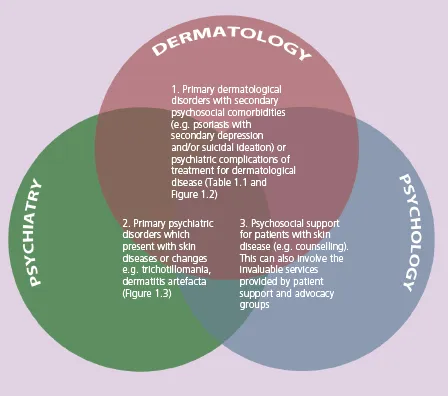
How do you help a dermatological patient with a psychological reaction? How do you differentiate psychological causes from true skin disease? These are challenges that ask dermatologists, psychiatrists, psychologists and other health care specialists to collaborate.
Practical Psychodermatology provides a simple, comprehensive, practical and up-to-date guide for the management of patients with psychocutaneous disease. Edited by dermatologists and psychiatrists to ensure it as relevant to both specialties it covers:
- History and examination
- Assessment and risk management
- Psychiatric aspects of dermatological disease
- Dermatological aspects of psychiatric disease
- Management and treatment
The international and multi-specialty approach of Practical Psychodermatology provides a unique toolkit for dermatologists, psychiatrists, psychologists and other health care specialists needing to care for patients whose suffering is more than skin deep.