1.1 Background
Schema Therapy (ST), developed originally for individual psychotherapy by Young (1990; Young, Klosko, & Weishaar, 2003), is an approach to the treatment of a wide variety of psychological disorders that integrates cognitive, experiential, or emotion-focused and behavioral pattern-breaking interventions. It is a comprehensive model that strategically integrates aspects of other approaches but remains unique. A group version of ST was developed (Farrell & Shaw, 2012; Reiss & Vogel, 2010; Muste, Weertman, & Claassen, 2009). The effectiveness of individual (IST) and group (GST) therapy for borderline personality disorder (BPD) has been validated empirically (Giesen-Bloo et al., 2006; Farrell, Shaw, & Webber, 2009; Reiss, Lieb, Arntz, Shaw, & Farrell, 2013a; Nadort et al., 2009). The model of ST is transdiagnostic. The use of ST for avoidant personality disorder (PD), social anxiety, eating disorders, post-traumatic stress disorder, narcissism, antisocial PD, substance abuse, and psychopathy is being explored and evaluated internationally. It is an approach that is rated positively by both patients and therapists (Spinhoven, Giesen-Bloo, van Dyck, Kooiman, & Arntz, 2007). In addition, ST has growing evidence of its cost-effectiveness for the individual modality (IST) (Giesen-Bloo et al., 2006; Nadort et al., 2009). However, the limited availability of specialized individual psychotherapies, including ST, in the current healthcare economy has prevented more wide-scale use of IST in clinical settings. An integrated program combining multiple GST sessions with a limited number of IST sessions in a structured program has been evaluated, with promising results (Muste, Weertman, & Claassen, 2009; Reiss et al., 2013a). Combining more frequent group ST sessions with strategically planned individual sessions has the potential for making this promising treatment more widely available in a larger number of settings.
The concept of an integrated and structured program was originally developed for use with severe patients in hospital settings (Reiss et al., 2013a), but it can be implemented across a wide range of patient populations, treatment settings, and treatment lengths. One patient population for whom it is ideal are those with personality disorders or PD features, those with chronic or complex psychological problems, those with multiple trauma histories, and those for whom other treatment approaches have failed. In general, these are patients who are treated at the higher levels of care and whose life potential is tragically not realized in the quality of their lives. An advantage of Schema Therapy is that it approaches treatment by targeting maladaptive schema modes rather than specific symptoms or disorders, thus transcending psychiatric diagnoses and impending changes in diagnostic classification. This program can be implemented in inpatient, day therapy, and intensive outpatient settings, as well as in general outpatient treatment with varying session frequency. A program of intensive sessions as the beginning of outpatient treatment may act to “jump-start” the treatment of patients with entrenched maladaptive coping strategies that produce the severe and sometimes life-threatening symptoms of disorders like BPD. It is possible to use all the handouts provided throughout this book within the context of individual ST treatment or selectively within other psychotherapy models. For example, the experiential interventions can augment cognitive therapy, filling a gap in that approach to treating patients with personality disorders and complex trauma.
The program of the manual is theoretically consistent with individual ST (Young et al., 2003) and group ST (Farrell & Shaw, 2012). Like most approaches to psychotherapy that go beyond skills training, ST requires specialized training to meet adherence and competence standards. This manual was designed to make IST, GST, and their integrated combination accessible for a wide range of psychotherapists of multiple theoretical orientations, including those working in intensive settings like inpatient and day therapy programs. The manual provides a detailed step-by-step guide for an ST fundamentals program that integrates IST and GST sessions. The program includes the core components of ST: limited reparenting, education about the ST model, mode awareness, mode management and cognitive, experiential, and behavioral pattern-breaking change work. It can be used across diagnostic groups. There are 12 individual sessions and 42 group sessions. Each session is described in terms of goals, therapist interventions, tips on management, sample session scripts for therapists to adapt, and corresponding information handouts, ST exercises, and therapy assignments. The individual sessions are designed to be complementary to the group work and the schema mode being focused on, while still allowing individual needs to be met. How to balance individual and group focus is discussed throughout. This level of detail will allow therapists new to Schema Therapy to conduct sessions with confidence and to coordinate group work effectively with individual work. It will also allow more experienced individual schema therapists to begin leading ST groups effectively. The program is not a rigid protocol, but rather a framework combining flexibility with standardization. The structured yet flexible format serves a number of purposes: the manual can be used as a detailed plan for implementing a structured, integrated program of individual and group ST in higher levels of care settings with multiple sessions per week; as a research protocol for psychotherapy outcome studies; or clinicians can select individual or group sessions, or the combination, to work on specific schema modes. Therapists can choose whether to implement the program as a whole, or to select individual sessions, group sessions, or a combination of both to suit their group and its needs.
1.2 The Chapters
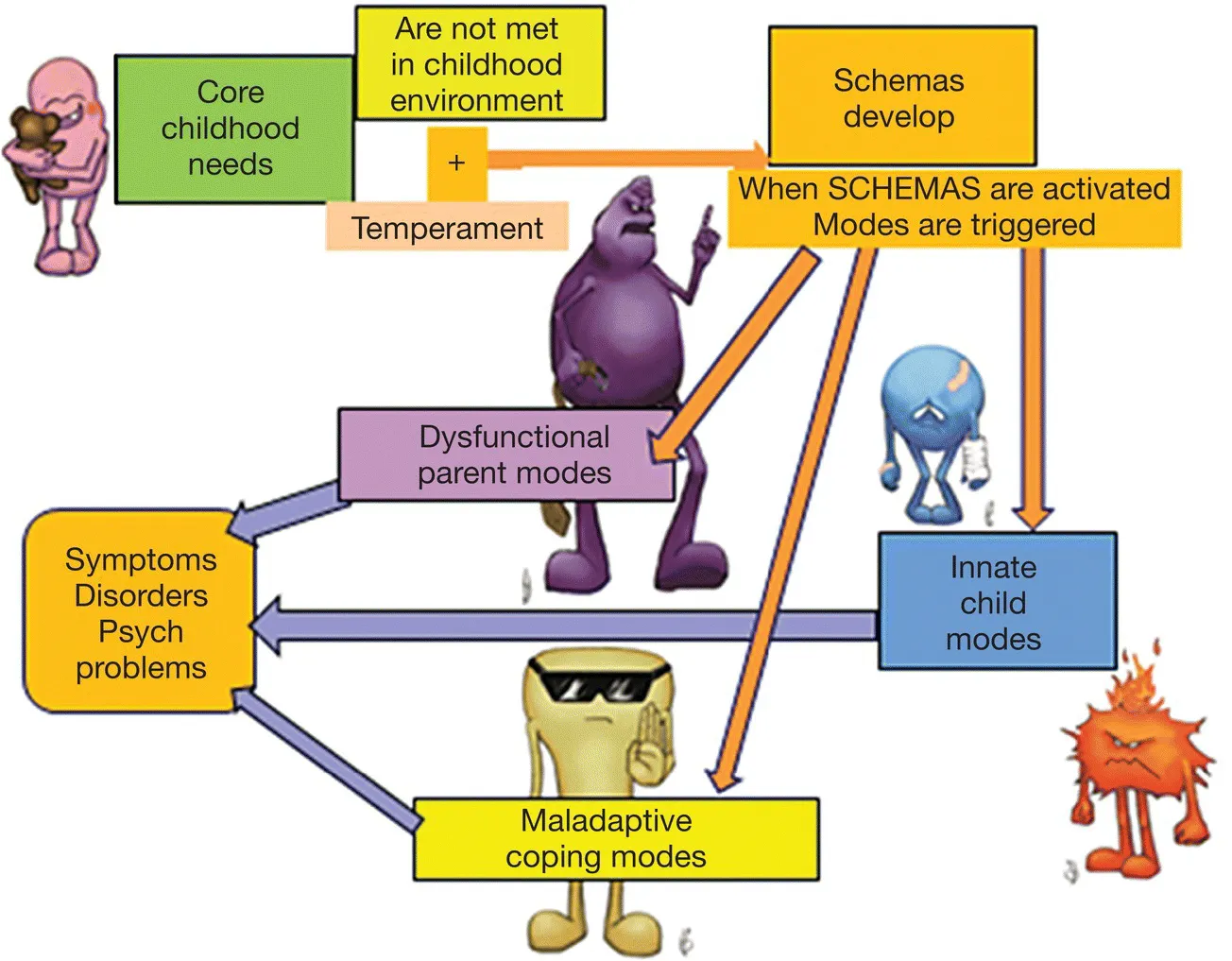
Chapter 2 presents the basic concepts of the ST model originally developed for individuals by Young (Young et al., 2003) and the adaptation for groups developed by Farrell and Shaw (2012). The goals of ST, the therapist approach of limited reparenting, and the core components of the model are described in this chapter. The approach of the integrated ST program to combining individual and group sessions is discussed. The general course and stages of the treatment program are outlined here. Chapter 3 describes some of the essentials of the treatment program: the patients, with inclusion and exclusion factors; the therapists; the milieu – both the physical setting and the multidisciplinary treatment team; the length of sessions and treatment; and the possible schedules and format for delivering the program in different settings. Chapter 4 presents the group sessions by component, with sample therapist scripts and the patient materials – handouts, group exercises, and session assignments. Chapter 5 presents the 12 individual sessions – with specific content, sample scripts, and handouts. Chapter 6 describes the ST training and supervision recommended for therapists. The research that has been conducted is summarized, with a brief description of the investigations that are in progress at the time of writing.
This book is unique in the ST literature as its goal is to provide an implementable program in its entirety. It is not focused on a particular disorder. It is not limited to one of the modalities of treatment delivery; it covers both individual and group ST. The reader is referred to the ST volumes in the References for theory and focus on specific disorders.